Archive : Article / Volume 2, Issue 1
- Research Article | DOI:
- https://doi.org/10.58489/2836-5917/007
Graft Flow Assessment with Transthoracic Doppler After Coronary Arterial Bypass Grafting with Bilateral Internal Thoracic Arteries
1Centre for Innovative Medical Biotechnology, Baltic Federal University, Kaliningrad, Russia
Tigran Akobyan, Centre for Innovative Medical Biotechnology, Baltic Federal University, Kaliningrad, Russia.
Tigran Akobyan, Graft Flow Assessment with Transthoracic Doppler After Coronary Arterial Bypass Grafting with Bilateral Internal Thoracic Arteries. Clin. Cardiol. Res. Vol. 2 Iss. 1. (2023) DOI: 10.58489/2836-5917/007
© 2023 Tigran Akobyan, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- Received Date: 06-02-2023
- Accepted Date: 16-02-2023
- Published Date: 28-02-2023
Transthoracic ultrasound; Internal thoracic arteries; Y-graft bypass grafting.
Abstract
Purpose — The aim of our study is to assess the transthoracic Doppler parameters of left internal thoracic artery`s stem (LITA) flow after coronary artery bypass surgery with free right internal thoracic artery using Y graft technique and compare them with such parameters of LITA-LAD (left anterior descending) graft flow after regular coronary artery bypass surgery (CABG).
Material and Methods — 51 consecutive patients with coronary artery disease underwent CABG. Comparison between groups was performed using the following parameters: age, body mass index, angina class, presence of hypertension and diabetes, left ventricular ejection fraction and haemoglobin level, hemodynamic parameters during the Doppler investigation.
Results — Higher systolic acceleration time value in Y graft group is due to bigger runoff of Y graft compared with the classic group. The diastolic acceleration time is shorter in Y graft group as the distal coronary runoff is bigger and LITA`s peak flow accelerates faster. The systolic and diastolic acceleration times are very sensitive parameters which depend on the distal coronary runoff changes.
Conclusions — We conclude that blood flow volume in tha LITA graft depend of coronary artery distal run-off and rising when we using to revascularize more than one coronary artery.
Introduction
The left internal thoracic artery (LITA) has proved to be an excellent conduit as a bypass graft because it has had a better long‐term patency rate than other grafts (saphenous vein, radial artery) [1, 2]. Angiography is considered the gold standard for graft assessment, however besides being an invasive and costly test, LITA angiography can be painful for the patient, adds to the risk contrast induced nephropathy. Non-invasive methods (like transthoracic Doppler) for assessment of LITA graft patency may be intermediate procedure before angiography and can preclude need of angiography. The role of recurrent graft Doppler assessment may be more important in patient after CABG (coronary artery bypass grafting) with angina and ECG ischemic changes on the left ventricular anterior wall leads [3, 4].
The new approach in CABG is total arterial revascularization, with both internal thoracic arteries using Y‐graft technique. Many surgeons recommended this method give the long term patency rate of internal thoracic arteries [5‐7].
The aim of our prospective study was to perform LITA`s stem flow evaluation after CABG, comparing data between groups of patients with only LITA to left anterior descending (LAD) grafts (named Classic or Conventional group) and bilateral internal thoracic arteries using Y‐graft technique (Y‐graft group).
Material and Methods
51 consecutive patients with coronary artery disease underwent CABG. The mean age was 53.6 years (range 32–71). Preoperative stable angina class I‐II (CCS) was in 3.9 % (n=2), stable angina class III‐IV in 11.8 % (n=6) and unstable angina in 84.3 % (n=43) patients. Hypertension present in 56.9 % (n=29) and diabetes mellitus in 21.6% (n=11) of patients.
Composite arterial Y‐grafting was performed using right internal thoracic artery (RITA) as a free graft attached to LITA in 17.6% (n=9) cases. LITA stem flow assessment was performed by transthoracic Doppler postoperatively. Doppler assessment of LITA stem flow was successful in 62.7% (n=32) patients.
Comparison between groups was performed using the following parameters: age, body mass index, angina class, presence of hypertension and diabetes, left ventricular ejection fraction and hemoglobin level, hemodynamic parameters during the Doppler investigation. All compared patients were male. The significant difference between groups was seen only by age, since we prefer to perform composite arterial grafting in young age patients to expect better long patency rate.
Operative Procedure
LITA was harvest as skeletonized conduit in all patients. Rigth internal thoracic artery (RITA) was harvested skeletonized as a free graft. The LITA graft was always anastomosed to the LAD. In 5 cases LITA was used for revascularization the diagonal branch also by side-to-side anastomosis. Composite Y-graft was constructed by anastomosing proximal end of RITA to LITA graft at the level of left atrial appendage before starting cardiopulmonary bypass. The RITA graft was used for revascularization the diagonal (n=1), intermedia (n=1), obtuse marginal (n=10) and posterior descending arteries (n=3). The distal and Y anastomoses in all of cases were performed with 8-0 polypropylene running suture.
Transthoracic Doppler
Thransthoracic Doppler assessment of the LITA`s stem flow (BIOSOUND A4 echo machine with 7.5 MHz linear transducer) was performed on the 7th day postoperatively. The scanner head was placed in the left upper parasternal space. It is well known that LITA`s stem flow type changes after surgery (diastolic flow becomes higher than systolic). The following flow parameters were measured and calculated: velocity flow integral (VFI), pulsating index (PI), resistance index (RI), peak velocity (Vp), mean velocity (Vm), flow acceleration (ACC), acceleration time (AT).
Statistical Methods
The dichotomic variables were compared by Chi square Pearson test, other variables which are not in normal distribution range assessed by Mann-Whitney U test. Outcomes showed in box-plot graphics.
Results
After comparing LIMA flow data in Y graft and classic groups we found the significant difference between the systolic flow acceleration time (AT) (Fig. 1), diastolic flow acceleration (dACC) (Fig. 2) and diastolic flow acceleration time (dAT) (Fig. 3).
It is known from the literature [9, 10] that Doppler evaluation of LIMA graft patentcy is performed by measuring and calculating peak velocity diastolo- systolic (dVp/Vp) (Fig. 4) and velocity flow integral diastolo-systolic ((dVFI/(dVFI+VFI)) x 100) ratios (Fig. 5). In our study we compared those parameters for both groups. No significant difference was found between two groups.
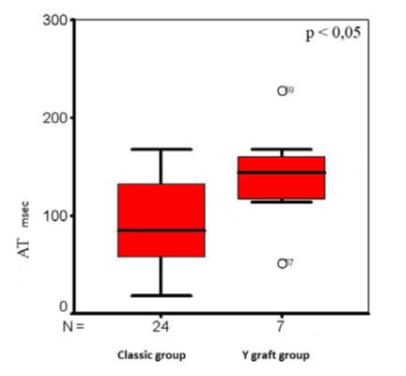
Figure. 1: The systolic flow acceleration times (AT)
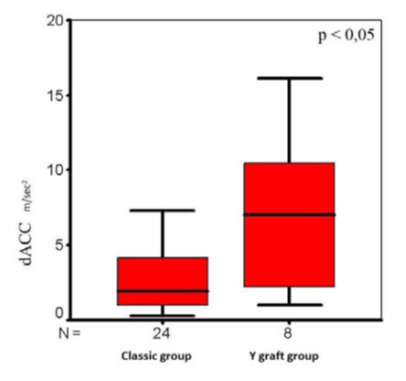
Figure 2: The diastolic flow acceleration (dACC) in groups
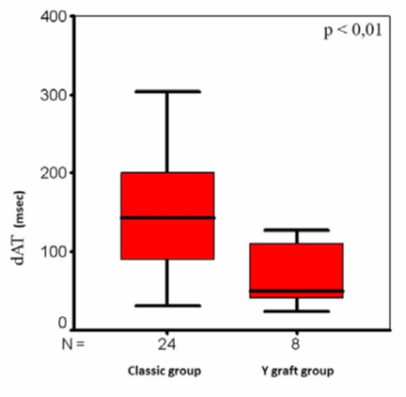
Figure. 3:The diastolic flow acceleration times (dAT) in groups
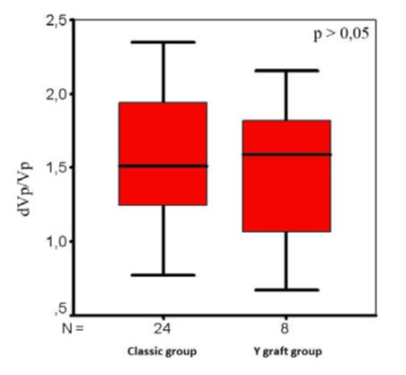
Figure. 4: The peak velocity diastolo‐systolic ratios in groups
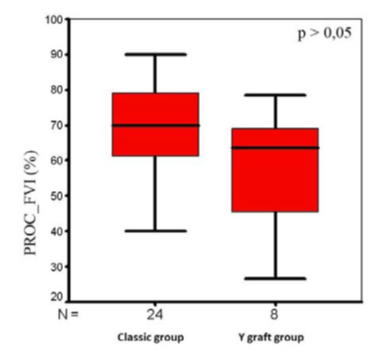
Figure. 5: The velocity flow integral diastolo‐systolic ratios in groups
Discussion
Normal graft flow type similar to conventional LITA- LAD graft flow type was observed in the Y graft group.
A major limitation of such flow studies is their incapacity to discriminate between the relative influence of the coronary arteriolar bed and that of the graft conduit itself. Even after a successful revascularization, the presence of some myocardial areas with resistive vessel damage or dysfunction resulting from previous episodes of ischemia or from surgery itself could affect the maximal blood flow. Interestingly, the values of postoperative flow reserve reported in all of these studies are lower than those reported previously in subjects without clinical evidence of coronary artery disease [8]. The independent LIMA graft displays a specific pattern of phasic flow with a transition from systolic- predominant to diastolic-predominant peak flow velocity shifting from the subclavian to the coronary end. This pattern was not confirmed in the Y-graft, in which we detected a diastolic-predominant peak flow velocity in the subclavian end. This peculiar flow pattern is probably related to the reduced vascular resistance of the parallel vascular circuit represented by the Y-graft configuration. Conversely, the independent LIMA graft displays a specific pattern of phasic flow with a transition from systolic- predominant to diastolic-predominant peak flow velocity shifting from the subclavian to the coronary end. This pattern was not confirmed in the Y-graft, in which we detected a diastolic-predominant peak flow velocity in the subclavian end. This peculiar flow pattern is probably related to the reduced vascular resistance of the parallel vascular circuit represented by the Y-graft configuration. Conversely, an impaired diastolic-predominant peak flow velocity in the proximal LIMA may presumably be the expression of high resistance in the RA limb of the Y-graft configuration [10].
Conclusion
We think that the higher systolic acceleration time in Y graft group is due to the bigger run off of the Y-graft as compared with the classic group. The diastolic acceleration time was shorter in the Y graft group since the total bypassed distal coronary run off diameter is bigger. This is the reason why the LITA`s peak flow achieves its maximal value in shorter time. So we think that the systolic and diastolic acceleration times, diastolic acceleration values changes with total bypassed coronary run off diameter. We conclude that blood flow volume in the LITA graft depend of coronary artery distal run-off and rising when we using to revascularize more than one coronary artery.
References
- Galbut, David L., Ernest A. Traad, Malcolm J. Dorman, Paul L. DeWitt, Parry B. Larsen, Deborah Weinstein, Joan M. Ally, and Thomas O. Gentsch. “Twelve-year experience with bilateral internal mammary artery grafts.” The Annals of thoracic surgery 40, no. 3 (1985): 264-270.
- Barner, Hendrick B., John W. Standeven, and Jeffrey Reese. “Twelve-year experience with internal mammary artery for coronary artery bypass.” The Journal of thoracic and cardiovascular surgery 90, no. 5 (1985): 668-675.
- Beard, J. D., D. J. A. Scott, J. M. Evans, R. Skidmore, M. Horrocks, R. Price, and J. A. Evans. “A Doppler flowmeter for use in vascular surgery.” In Proc Biol Eng Soc, vol. 4, pp. 6-12. 1988.
- Fujiwara, T., F. Kajiya, S. Kanazawa, Shuji Matsuoka, Y. Wada, O. Hiramatsu, M. Kagiyama, Y. Ogasawara, K. Tsujioka, and T. Katsumura. “Comparison of blood-flow velocity waveforms in different coronary artery bypass grafts. Sequential saphenous vein grafts and internal mammary artery grafts.” Circulation 78, no. 5 (1988): 1210-1217.
- Tector, Alfred J., Monica L. McDonald, David C. Kress, Francis X. Downey, and Terence M. Schmahl. “Purely internal thoracic artery grafts: outcomes.” The Annals of thoracic surgery 72, no. 2 (2001): 450-455.
- Calafiore, Antonio Maria, Marco Contini, Giuseppe Vitolla, Michele Di Mauro, Valerio Mazzei, Giovanni Teodori, and Gabriele Di Giammarco. “Bilateral internal thoracic artery grafting: long-term clinical and angiographic results of in situ versus Y grafts.” The Journal of thoracic and cardiovascular surgery 120, no. 5 (2000): 990-998.
- Muneretto, Claudio, Alberto Negri, Jacopo Manfredi, Alberto Terrini, Giulia Rodella, Suad ElQarra, and Gianluigi Bisleri. “Safety and usefulness of composite grafts for total arterial myocardial revascularization: a prospective randomized evaluation.” The Journal of thoracic and cardiovascular surgery 125, no. 4 (2003): 826-835.
- Glineur, David, Philippe Noirhomme, Jim Reisch, Gebrine El Khoury, Parla Astarci, and Claude Hanet. “Resistance to flow of arterial Y-grafts 6 months after coronary artery bypass surgery.” Circulation 112, no. 9_supplement (2005): I-281.
- Orihashi, Kazumasa, Taijiro Sueda, Kenji Okada, and Katsuhiko Imai. “Left internal thoracic artery graft assessed by means of intraoperative transesophageal echocardiography.” The Annals of thoracic surgery 79, no. 2 (2005): 580-584.
- Mannacio, Vito, Luigi Di Tommaso, Vincenzo De Amicis, Francesco Musumeci, and Paolo Stassano. “Serial evaluation of flow in single or arterial Y-grafts to the left coronary artery.” The Annals of thoracic surgery 92, no. 5 (2011): 1712-1718.


