Archive : Article / Volume 2, Issue 1
- Case Report | DOI:
- https://doi.org/10.58489/2836-5917/009
Fentanyl Overdose Presented with Unconsciousness, Hypoxia, Hypotension and Pinpoint Pupil Complicated by Acute Kidney Injury and Right Hemiparesis: A Rare Case Report
1Professor and Head/ Senior Consultant Physician, Department of Medicine/ Department of Nephrology, Defence Services Medical Academy/ No. [1] Defence Services General Hospital (1000 Bedded)
2Consultant Physician, No. [1] Defence Services General Hospital, (1000 Bedded)
3Assistant Lecturer, Department of Medicine, Defence Services Medical Academy
4Consultant Intensivist, No. [1] Defence Services General Hospital, (1000 Bedded)
5Consultant Radiologist, No. [1] Defence Services General Hospital, (1000 Bedded)
Khin Phyu Pyar, Professor and Head/ Senior Consultant Physician, Department of Medicine/ Department of Nephrology, Defence Services Medical Academy/ No. [1] Defence Services General Hospital (1000 Bedded)
Khin Phyu Pyar, et, al. Fentanyl Overdose Presented with Unconsciousness, Hypoxia, Hypotension and Pinpoint Pupil Complicated by Acute Kidney Injury and Right Hemiparesis: A Rare Case Report. Clin. Cardiol. Res. Vol. 2 Iss. 1. (2023) DOI: 10.58489/2836-5917/009
©2023 Khin Phyu Pyar, this is an open-access article distributed under the creative commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cite
- Received Date: 07-04-2023
- Accepted Date: 20-05-2023
- Published Date: 26-04-2023
Fentanyl overdose, Unconsciousness, Pinpoint pupil, Acute kidney injury, Right hemiparesis, Multiple cerebral infarction.
Abstract
A 25-years-old -male was found unconscious with empty fentanyl ampule; slow breathing with central cyanosis; SaO2 85% on air; blood pressure 90/50 mmHg, pulse rate 100/minutes; respiratory rate 12/minutes; central cyanosis; crackles in both lungs; multiple venipuncture marks in his left forearm and pinpoint pupil. He was treated as fentanyl overdose with intravenous naloxone, fluid therapy, ventilatory support and oxygenation. Right hemiparesis was noted on recovery; CT scan head showed multiple areas of infarction in basal ganglia and cerebral hemisphere. Acute kidney injury recovered with hemodialysis.
Introduction
WHO highlights the epidemics of opioids “half million deaths are attributable to drug use. More than 70% of these deaths are related to opioids, with more than 30% of those deaths caused by overdose [13,10]. Fentanyl is a synthetic opioid; it is 50 times stronger than heroin and 100 times stronger than morphine. More than 75% of drug overdose cases were due to fentanyl. Typical features of fentanyl overdose are similar to morphine; pinpoint pupil, respiratory depression, central cyanosis, falling conscious level with venipuncture marks are clues for diagnosis. The signs and symptoms respond quickly to parenteral naloxone; severe cases may need ventilatory support. Drug addicts commonly take more than one drug with or without alcohol. Commonly reported drugs presenting with acute overdose to emergency department are fentanyl, morphine, pethidine, marijuana amphetamine, benzodiazepine [4]. Drug addiction was associated with cerebrovascular accident particularly in those without risk factors for stroke like diabetes mellitus, hypertension and young age [12,5]. Features of cerebral infarction was detected in computed tomography of brain in patient with overdose of opioids and benzodiazepine and it was related with hypoxic brain injury [2]. Bilateral basal ganglia lesions were suggestive of narcotic overdose in unconscious patient [7].
Case Presentation
A twenty-five-year-old OT nurse was found unconsciousness by his friends in his room as he did not turn up to his duty. A syringe with empty ampule of fentanyl was found beside him. There were multiple venipuncture marks in his left forearm; he was righted person. He was unconscious (Glasgow Coma Score 3/15); hypoxic; SaO2 85% on air; blood pressure 90/50 mmHg, pulse rate 100/minutes; respiratory rate 12/minutes; central cyanosis; crackles in both lung and pinpoint pupil. He was treated as a case of narcotic over dose. Initial resuscitation was done; oxygenation, ventilatory support, intravenous fluids and naloxone. Then, he regained consciousness (Glasgow Coma Score 13/15). In view of pinpoint pupil, tachycardia and labile blood pressure, brain stem hemorrhage was suspected though there was neither fever nor projectile vomiting; urgent CT scan of head was done. The brain stem was normal; however, areas of infarction were seen in basal ganglia and cerebral hemisphere. Later, the patient developed acute kidney injury; oliguria, raised serum creatinine, hyperkalemia and metabolic acidosis. Therefore, hemodialysis was done; he became fully conscious and orientated (Glasgow Coma Score 15/15). When he regained consciousness, motor system examination was done; motor power on right lower limb was 4/5 with extensor planter response. CT scan of head was repeated and it showed multiple areas of infarction on left cerebral hemisphere and basal ganglia more on left side

Figure 1: Multiple venipuncture marks in left cubital fossa
Discussion
Opioids overdose is an increasing problem world-wide; there is an acceleration of overdose deaths during the COVID-19 pandemic. Overdose deaths involving synthetic opioids in 2020 was nearly 20 times the number in 2013. This patient presented with typical features of narcotic overdose; pinpoint pupil, respiratory depression, central cyanosis, falling conscious level with venipuncture marks which responded dramatically to naloxone. It highlights the awareness of opioids overdose in Myanmar as early diagnosis and antidote treatment prevent death. Because opioids addition is an increasing problem world-wide this patient may be one of “Ice-burg phenomenon”. Fentanyl is relatively cheap among opioids; therefore, it is more affordable. In addition, it is 50-100 times stronger than heroin and morphine making high addictive potency. Therefore, the prevalence of fentanyl addiction would be increasing trend in the future. This case report might improve public health awareness. Drug addicts commonly take more than one drug with or without alcohol. This patient did not admit drug abuse though empty fentanyl ampule was found next to him. His blood analysis confirmed marijuana. His clinical presentation was consistent with narcotic overdose; it made excellent recovery with naloxone. Hence, this patient confirmed the fact that “drug addicts commonly take more than one drug with or without alcohol”. Cerebrovascular accident was not commonly associated with narcotic addiction [12,11]. cerebral hemorrhage with amphetamine [3]. and cerebral infarction with opioids [11,12]. This patient was 28 years old and he had left hemiparesis. It pointed out that “the causes of young stroke may be narcotic addiction”. This patient had left hemiparesis and CT scan of brain revealed cerebral infarct at cerebral hemisphere and basal ganglia. It confirmed previous report “bilateral internal capsule hypoglycemics and bilateral frontal lobe infarction was detected in computed tomography (CT) of brain in patient with overdose of opioids and benzodiazepine [2]. The outcome of patients with narcotic overdose and abnormal CT scan findings was not good in previous findings although this patient was lucky. Twenty percent of patients with acute opium overdose had abnormal brain CT findings (infarct / ischemia); and they had poor prognosis in one report [8]. This is one reason for doing case report. Hypoxic ischemic brain injury were commonly seen in patients with opioid abuse [1]. In this patient, abnormal brain CT findings was bilateral basal ganglia hypodensities and multiple hypodensities scattered in the cerebral hemispheres. Hassan recommended that the presence of bilateral basal ganglia lesions in brain CT in should alert the physician of opioid use disorder [6]. If bilateral basal ganglia lesions were found in brain CT, the etiology of unconscious patients would be opioid use disorder. This is another learning point from this patient “association between narcotic overdose and brain imaging”
Conclusion
Fentanyl overdose should be suspected if patient has altered conscious level, pinpoint pupil, cyanosis, respiratory depression and needle marks. It may result in cerebral infarction; cerebrovascular accident. Basal ganglia infarction in CT scan of head in unconscious patient is likely to be due to opioid use disorder. It is important to recognize, treat and prevent fentanyl overdose which is going to be epidemic form in the future.

Figure 2: CT head showing cerebral infarction.
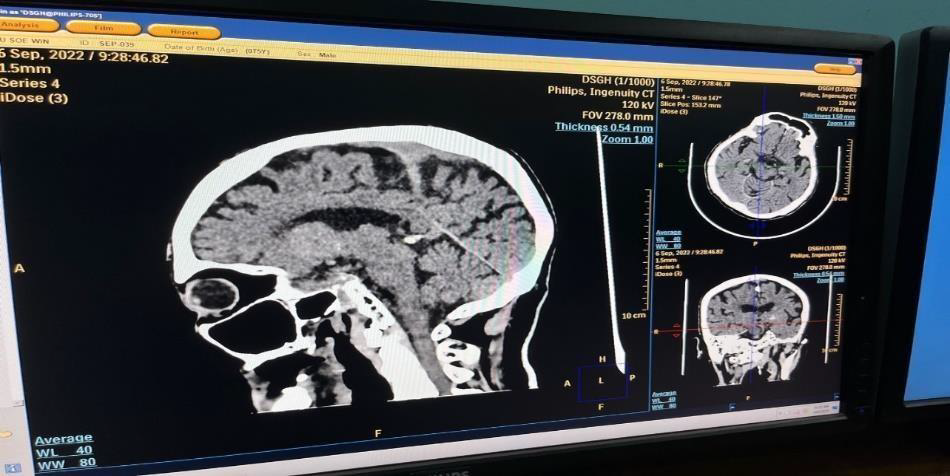
Figure 3: CT head showing basal ganglia infarction

Figure 4: CT head showing bilateral basal ganglia infarction.
Acknowledgements
The authors would like to thank the patient for giving consent to this article. Also, to all doctors and nursing team for making great efforts in caring him. The authors acknowledged the following team; Professor Tin Moe Mya for laboratory support, Professor Myint Zaw, Professor Kyaw Zay Ya and Professor ’Ko Ko Lwin’ for administrative support
Declaration of conflict of Interest
The authors declared no potential conflicts of interests with respect to authorship and publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting cases.
Funding
The authors received no financial support for publication of this article.
Informed consent
The informed consent for publication in this article was obtained from patient.
References
- Bates, David DB, Katherine Gallagher, HeiShun Yu, Jennifer Uyeda, Akira M. Murakami, Bindu N. Setty, Stephan W. Anderson, and Mariza O. Clement. “Acute radiologic manifestations of America’s opioid epidemic.” Radiographics 38, no. 1 (2018): 109-123.
- Butt, M. U., and Reeja Nadir. “An Unusual Presentation of Opioid Induced Cerebral Infarction.” Journal of the College of Physicians and Surgeons--pakistan: JCPSP 26, no. 6 Suppl (2016): S76-8.
- Buxton, Neil, and Norman S. McConachie. “Amphetamine abuse and intracranial haemorrhage.” Journal of the Royal Society of Medicine 93, no. 9 (2000): 472-477.
- Glick, Jennifer L., Tricia Christensen, Ju Nyeong Park, Michelle McKenzie, Traci C. Green, and Susan G. Sherman. “Stakeholder perspectives on implementing fentanyl drug checking: Results from a multi-site study.” Drug and alcohol dependence 194 (2019): 527-532.
- Ochoa, SA Gómez. “Stroke and cannabis use in patients with no cardiovascular risk factors: a systematic review of case reports.” Neurología (English Edition) 36, no. 3 (2021): 222-228.
- Hassan, Ali, Mahdi Al Jawad, Amna Alsaihati, Haitham Alaithan, and Faisal Al Hawaj. “Bilateral basal ganglia lesions in patients with heroin overdose: a report of two cases.” Case Reports in Acute Medicine 2, no. 3 (2020): 62-68.
- Hassan, Ali, Mahdi Al Jawad, Amna Alsaihati, Haitham Alaithan, and Faisal Al Hawaj. “Bilateral basal ganglia lesions in patients with heroin overdose: a report of two cases.” Case Reports in Acute Medicine 2, no. 3 (2020): 62-68.
- Jamshidi, Farkhondeh, Babak Sadighi, Kamran Aghakhani, Hossein Sanaei-Zadeh, Mohammadali Emamhadi, and Nasim Zamani. “Brain computed tomographic scan findings in acute opium overdose patients.” The American journal of emergency medicine 31, no. 1 (2013): 50-53.
- Janszky, Imre, Ioannis Vardaxis, Bo Henry Lindqvist, Jens Wilhelm Horn, Ben Michael Brumpton, Linn Beate Strand, Inger Johanne Bakken et al. “Assessing short-term risk of ischemic stroke in relation to all prescribed medications.” Scientific Reports 11, no. 1 (2021): 21673.
- Jiang, Xinyi, Gery P. Guy Jr, Christopher Dunphy, Cassandra M. Pickens, and Christopher M. Jones. “Characteristics of adults reporting illicitly manufactured fentanyl or heroin use or prescription opioid misuse in the United States, 2019.” Drug and alcohol dependence 229 (2021): 109160.
- Ortiz, Juan Fernando, Claudio Cruz, Amrapali Patel, Mahika Khurana, Ahmed Eissa-Garces, Ivan Mateo Alzamora, Taras Halan, Abbas Altamimi, Samir Ruxmohan, and Urvish K. Patel. “Opioid antagonist in the treatment of ischemic stroke.” Brain Sciences 11, no. 6 (2021): 805.
- Uhegwu, Nnamdi, Asif Bashir, Mohammed Hussain, Haitham Dababneh, Sara Misthal, and Aaron Cohen-Gadol. “Marijuana induced reversible cerebral vasoconstriction syndrome.” Journal of Vascular and Interventional Neurology 8, no. 1 (2015): 36.
- World Health Organization. (2021, August 4). Opioid overdose


