Archive : Article / Volume 2, Issue 2
- Research Article | DOI:
- https://doi.org/10.58489/2836-5917/011
4Dimensional XStrain Echocardiography: M-mode and Tissue Doppler Estimation of Age and Gender Specific Normative Values of Aortic Stiffness in Healthy Adults during Covid-19 Pandemic
1Chief, Non-Invasive Cardiologist, Pediatric and Adult Cardiology, Prakash Heart Station
2Department of Cardiology, Star Hospital, Hyderabad, India
3Lead - PMO, Tech Mahindra, Noida, Uttar Pradesh, India
Akhil Mehrotra, Chief, Non-Invasive Cardiologist, Pediatric and Adult Cardiology, Prakash Heart Station.
Shubham Kacker, Amarnath Patnaik, Akhil Mehrotra . 4Dimensional XStrain Echocardiography: M-mode and Tissue Doppler Estimation of Age and Gender Specific Normative Values of Aortic Stiffness in Healthy Adults during Covid-19 pandemic.”. Clin. Cardiol. Res. Vol. 2 Iss. 2. (2023) DOI: 10.58489/2836-5917/011
© 2023: Akhil Mehrotra, this is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
- Received Date: 30-05-2023
- Accepted Date: 07-06-2023
- Published Date: 03-07-2023
Aortic Stiffness, Aortic elasticity, 4D XStrain echocardiography, TDI of Aorta, Healthy adults, Covid-19 pandemic.
Abstract
The elastic properties of the aorta are modified in numerous cardiovascular and non-cardiovascular diseases. Multiple studies have evaluated aortic stiffness in myriads of disease state, albeit only few Indian studies have estimated the normal values of aortic stiffness in healthy population. To the best of our knowledge, till date no research has been undertaken to determine the age and gender specific value ranges of aortic stiffness parameters in healthy subjects. Hence, in the present study we endeavoured to estimate these values in our distinctive study groups of healthy adults. This was a prospective observational study in which 58 healthy adults were enrolled during the turbulent corona pandemic. Study group was of the age group 18-60 years of either sex and was arbitrarily divided into six groups. Exhaustive M-mode and Tissue doppler Imaging was performed by 4Dimensional XStrain echocardiography system for extensive evaluation of multiple M-mode and Tissue Doppler imaging derived parameters of Aortic stiffness and superior wall velocities of ascending aorta. AOS, AOD, Aortic strain, and elasticity modulus were greater in males. On the contrary Aortic superior wall velocities (SAO, EAO, and AAO) were higher in females. Increasing age led to a decline in majority of stiffness parameters derived by M-mode echocardiography. Correspondingly EAO determined by TDI of superior wall of aorta, showed a deterioration with advancing age. The authors report a normal range of M-mode and TDI derived values of Aortic stiffness of ascending aorta, in healthy Indian adults. Difference in magnitude of aortic elasticity indices has been demonstrated in men and women, as well as in different subsets of the study group.
Introduction
Functional properties of the aorta are major determinants of normal cardiovascular (CV) function [1]. Increments in aortic stiffness and reduction in aortic distensibility (indicators of elastic properties of aorta) are associated with coronary artery disease [2,3]. Aortic elasticity is an established methodology for risk stratification of atherosclerotic heart disease, myocardial infarction, stroke and heart failure [3].
Numerous methods have been employed for the evaluation of aortic elasticity, namely magnetic resonance imaging (MRI), aortic angiography applanation tonometry, velocity vector imaging, and gated radionuclide angiography [4-8]. Moreover M-mode and Tissue Doppler Imaging (TDI) of the ascending aorta is also used to estimate its elastic properties [9-14].
The elastic properties of the aorta are modified in numerous CV and non-cv diseases. Hypertension, mitral valve prolapses, aortic aneurysms, coronary artery disease and heart failure, being the major cv disease and cystic fibrosis, pregnancy, chronic kidney disease, hypothyroidism, sarcoidosis, al-antitrypsin deficiency and diabetes, being the non-cv diseases, altering the aortic stiffness properties [15-24].
Even though aortic stiffness has been evaluated in myriads of disease states, in contrast only few Indian studies have assessed the normal values of aortic stiffness parametersin healthy population [25,26]. Till date, no research has been undertaken to determine the age and gender specific value ranges of aortic stiffness parameters in healthy subjects. Hence, in the present study we endeavoured, to determine the above-mentioned normative values in our distinctive study groups of healthy population.
Material and Methods
This study was carried out at Prakash Heart Station and Diagnostic centre, Lucknow, India. This was prospective, observational study in which 258 healthy Indian adults were recruited, and later on, 200 cases were omitted due to inferior image quality. Finally, 58 participants were enrolled during a period of 9 months from September 2021 to May 2022. Study group was of the age group 18-60 years of either sex, and was arbitrarily divided into six groups:
1. Group A- Overall study population subjects from 18-30 years of age.
2. Group B- Overall study population subjects from 31-60 years of age.
3. Group C- Male subjects from 18-30 years of age
4. Group D- Female subjects from 18-30 years of age
5. Group E- Male subjects from 31-60 years of age
6. Group F- Female subjects from 31-60 years of age
Those participants were included, if they were asymptomatic with a normal physical examination BMI-23 or less, waist size 85 cm2 or less in men and 80 cm2 or less in women, free from overt cardiovascular disease, not receiving any drugs, nonsmoker, nontobacco chewer, nondiabetic, non-hypertensive according to JNC-8 guidelines, having normal thyroid and lipid profile, normal resting electrocardiogram (ECG) in sinus rhythm with a normal two-dimensional echocardiography and Treadmill Stress ECG. Those individuals were excluded if there was presence of diabetes mellitus, neurological or psychiatric illness, malignancy, CAD, Aortic root abnormalities and aortic dilatation thyroid disease, valvular heart disease, history of cardiac rhythm abnormalities, heart failure, systemic hypertension, and significant pulmonary hypertension.
The study procedure was approved by the Institutional Ethics Board of Prakash Heart Station and Diagnostic, Lucknow, India. All subjects or their guardians gave their written informed consent prior to data collection and furthermore confidentiality of patient information was maintained.
Data collection and study procedure
All patients underwent full history taking, clinical examination, and a standard resting 12-lead ECG. A negative Covid-19 reverse transcription polymerase chain reaction report was conducted within 72 h prior to the date of enrollment and echocardiography, was the essential requirement because the study was conducted during the raging Covid-19 pandemic.
Biochemical and Hormonal Assessment
After 12 h of overnight fasting, blood samples were withdrawn for HBAIC, T3T4TSH, Serum creatinine, Total cholesterol, Triglycerides, low-density cholesterol, and high-density cholesterol. These estimations were done to rule out the presence of diabetes mellitus, hypothyroid or hyperthyroid state, renal failure, and dyslipidemia.
Blood pressure measurement
Blood pressure (BP) levels were measured from the right brachial artery at the level of the heart with a mercury sphygmomanometer after resting for at least 5 minutes in the supine position. Three measurements, at least 2 minutes apart, were performed, and the average of the closest two readings was recorded. A pressure drop rate of approximately 2 mm Hg/S was applied, and Korotkoff ’s phases I and V were used for systolic and diastolic BP (SBP and DBP, respectively) levels. All BP measurements were made by a cardiologist. Pulse pressure (PP) was calculated as systolic minus diastolic BP.
Echocardiography
All echocardiographic evaluations were performed by the author, using- MyLab X7 4D XStrain echocardiography machine, Esaote, Italy. The images were acquired using a harmonic variable frequency (1- 5 Mhz) electronic single-crystal array transducer with the subject lying in the left lateral decubitus position.
Conventional Echocardiography
M-mode, 2-Dimensional, and pulsed wave doppler (PWD) echocardiography was performed from parasternal long-axis, short-axis, and apical 3 chamber, 4 chamber, and 2 chamber views, and the following data were derived: Interventricular septum thickness in diastolic and systolic (IVSd and IVSs respectively), left ventricular posterior wall thickness in diastole and systole (LVPWd and LVPWs, respectively), left ventricular end-diastole and end-systole volumes (LVEDV and LVESV, respectively). Moreover, 2- Dimensional ejection fraction (2D-EF %) by biplane Simpson’s method, LV mass in diastole (LV Mass d), and cardiac output (CO) were also determined. Cardiac Index was calculated by dividing the CO by body surface area (BSA). By using PWD, early diastolic velocity (E), late diastolic velocity (A), and E/A ratio were measured.
Aortic stiffness assessment by M-mode echocardiography of Ascending Aorta
Systolic and diastolic inner diameter of ascending aorta Systolic and diastolic inner diameters of ascending aorta were recorded by M-Mode echocardiography 3 cm above the aorta valve in a parasternal long-axis image. Aorta systolic diameter (AOS) was measured at the maximum anterior motion of the aorta, and aorta diastolic diameter (AOD) was measured at the peak of the QRS complex on the recorded ECG. (Figure 1, 2). All the parameters were computed and the average of 5 consecutive cycles were calculated.
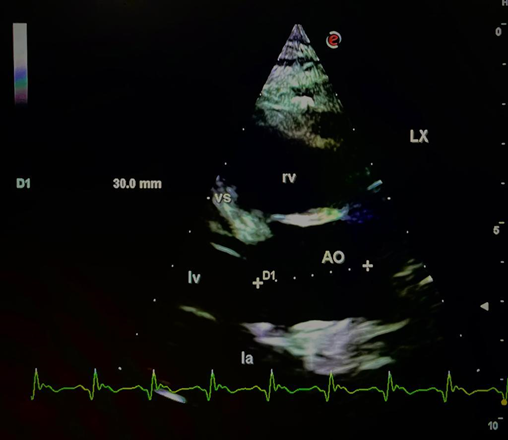
Figure 1: Measurement of aortic diameter obtained at 3 cm above the aortic cusps
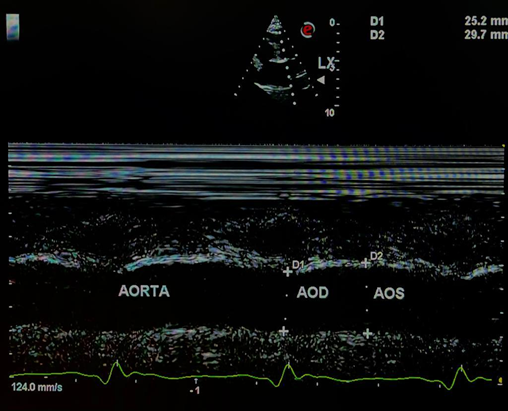
Figure 2: Aorta visualized on M- mode. The movement of aortic wall appears as two wavy lines. The space between the two lines is the aortic lumen. Systolic and diastolic diameters are measured on M- mode.
Aortic distensibility (D), aortic stiffness index (SI) and other elasticity parameters were determined by using the following formulas [27,28].
1. aortic Distensibility = 2x AOS–AOD/[(SBP–DBP) X AOD (106. cm2 dyn-1)]
2. Aortic Stiffness Index = ln (SBP/DBP)/ [AOS – AOD]/AOD] (pure number), ln = natural logarithm
3. Aortic Pulsatile Change (APC) = AOS – AOD (cm)
4. Aortic Systolic index (ASysI)
5. Aortic Diastolic Index (ADI)
6. Aortic pulsatile index (API)
ASysI, ADI, and API were calculated by dividing AOS, AOD and APC by body surface area (BSA), respectively
1. Aortic compliance (AS) = (AOS-AOD/SBP-DBP) (cm/mmHg)
2. Elasticity Modulus (EM) = (SBP-DBP)/([AOS- AOD]/AOD) (Pa)
3. Aortic strain (AS) = (SAO - AOD) X100/ AOD (%)
Tissue Doppler imaging of Ascending Aorta
Aortic upper-wall velocities were measured by Tissue Doppler Imaging (TDI) at the same point as in the M- mode measurements (Figure 3) gain and filter were adjusted to optimize the image. High temporal resolution (>100 frames/s) and a sweep speed set to
100 mm/s were used. The TDI of expansion peak velocity during systole (SAO) and early (EAO) and late (AAO) contraction peak velocities during diastole were obtained with a 1-mm sample volume size
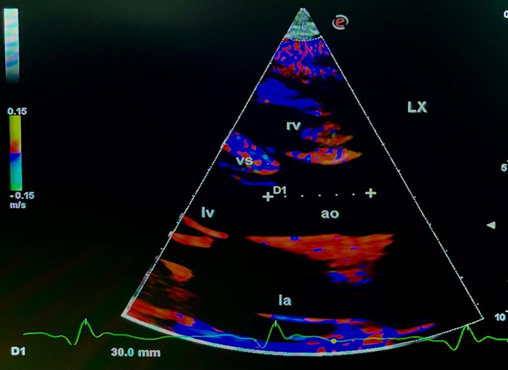
Figure 3: Tissue Doppler Imaging of the ascending aorta. The measurements were made at a level of 3 cm above the aortic cusps, at the same point as that for M-mode echocardiography.
The resulting velocities were recorded for 5 consecutive cardiac cycles and stored for later playback and analysis.
Following data were estimated by TDI of the superior wall of ascending aorta (Figure 4).
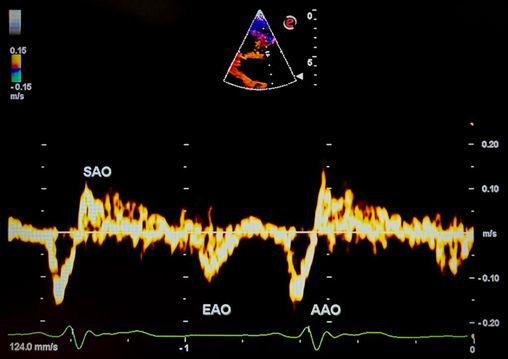
Figure 4: Aortic superior wall velocity measurements with tissue doppler imaging. SAO, systolic superior wall velocity, EAO, early diastolic superior wall velocity, AAO, late diastolic superior wall velocity.
1. SAO- Aortic superior wall velocity in systole was calculated at the same point used in M-mode measurement.
2. EAO- Early diastolic velocity
3. AAO- Late diastole velocity
Tissue Doppler Echocardiography of the left ventricle
TDI of LV was conducted by placing the PWD sample volume at the lateral mitral annulus in apical four- chamber view, and early diastolic velocity (E’) and E/E’ ratio were determined in the TDI mode.
Four-dimensional XStrain speckle-tracking echocardiography
From the apical position, two-dimensional cine loops were acquired from two-chamber, three-chamber, and four-chamber views. A high-quality ECG signal was a must for proper gating, and a minimum of three cardiac cycles were acquired for each cine loop. The study was performed with a frame rate between 40 and75 fps and then stored digitally on a hard disk for offline analysis by software package XStrainTM advanced technology TOMTEC GMGH 3D/4D rendering BeutelTM computation capabilities (Figure 5) [29].
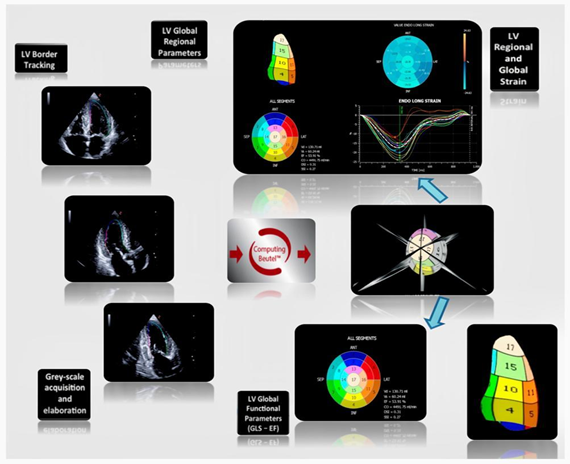
Figure 5: XStrain 4D global LV analysis. At the end of each scanning section, the three apical views are acquired. Then, after left ventricular (LV) endocardial border tracking, the software analyzes LV regional deformation parameters. Finally, the Beutel 3D reconstruction allows quantification of global LV function (global longitudinal strain (GLS)—ejection fraction). XStrainTM 4D.
The LV endocardial and epicardial borders were identified, tracked, and highlighted by a semiautomatic tool-AHS Aided Heart segmentation Esaote, for border segmentation. Thirteen equidistant tracking points were automatically incorporated along the LV endocardial border and where necessary manual adjustment of endocardial tracing was done. The software automatically divided the LV wall into 6 segments and them the acquired cine loop of each apical view was tracked frame by frame throughout the entire cardiac cycle. The cine loops with inadequate tracing quality and with any signs of arrhythmia were excluded.
The LV bull’s eye depiction according to 17-segment model was generated by XStrain 4D software, by integrating the results of each set of cine loops [30,31].
XStrain-4D software created a 3D reconstruction for calculating LV volumes and EF [32], and XStrain 4D-EF by the “Beutel Mode” method (TOMTEC, Germany) (Figure 6) [33].
The following 4D XStrain estimated values of volumetric values were statistically analyzed.
• Volumetric data: Sphericity index in diastole and systole, LVEDV, LVESV, 4D-EF%, and CO.

Figure 6: XStrain 4D software created a 3D reconstruction for calculating LV volumes and XStain 4D-EF by the “Beutel Mode” method (TOMTEC, Germany).
Statistical Analysis
Statistical analysis was performed with the Microsoft excel® (Excel 2019. Microsoft Corp; Seattle Washington. USA). The continuous variables are expressed as mean ± SD. The 95% confidence interval of the mean was also calculated. Enrolled participants were stratified according to Groups A-F, age: < 30 years and > 31 years, and gender: male and female. Comparison of various datasets between men and women and between different age groups was performed by Students t-test for independent groups.
The level of significance used was <0.05. A higher t value having a probability <0.05 was marked significant. A p-value <0.01 was marked as highly significant.
Result
We performed Aortic stiffness assessment of ascending aorta in 58 healthy Indian adults of age 18-60 years mean 32.16 ± 11.82 years, free from overt cardiovascular disease (Table 1). The study population was arbitrarily divided into six groups: Group A from 18-30 years of age, Group B from 31-60 years of age, Group C, male subjects of 18-30 years, Group D, female subjects of 18-30 years, Group E, male subjects of 31-60 years and Group F, female participants of 31-60 years.
|
Variables
|
Study Population (n:58)
|
Male(N-38)
|
Female(N-20)
|
|
Mean ± SD
|
Mean ± SD
|
||
|
Age (yrs)
|
32.16 ± 11.82
|
30.53 ± 12.22
|
35.25 ± 10.61
|
|
Weight (kg)
|
61.45 ± 11.08
|
64.18 ± 10.44
|
56.25 ± 10.62
|
|
Height (cm)
|
164.45 ± 8.62
|
167.42 ± 6.84
|
158.80 ± 8.99
|
|
BSA (m2)
|
1.67 ± 0.18
|
1.72 ± 0.16
|
1.57 ± 0.18
|
|
BMI
|
22.56 ± 2.66
|
22.77 ± 2.52
|
22.17 ± 2.93
|
|
SBP (mm Hg)
|
118.28 ± 10.97
|
118.26 ± 10.58
|
118.30 ± 11.95
|
|
DBP (mm Hg)
|
76.66 ± 6.58
|
76.74 ± 6.60
|
76.50 ± 6.71
|
|
Heart Rate (bpm)
|
80.45 ± 14.52
|
77.89 ± 13.06
|
85.30 ± 16.21
|
Table 1: Demographic Data (n=58)
NS=Not Significant(p>0.05),** Highly Significant=(p<0 Significant=(p>
Demographic data
The mean BSA of the participants was 1.67±0.18 sq.metre. There were 38 males and 20 females with a mean age of 30.53±12.22 years and 35.25±10.61 years respectively, and a mean BSA of 1.72±0.16 sq.metre, and 1.57±0.18 sq.metre respectively (Table 1). The mean age in Group A-E was 23.13±4.33 years, 42.52±8.71 years, 21.68±3.95 years, 26.66±3.08 years, 42.68±8.61 years and 42.27±9.25 years respectively and mean BSA was 1.64±0.17m2, 1.40±0.2m2, 1.67±0.14m2, 1.56±0.18m2, 1.78±0.16m2, 1.56±0.17m2,
respectively (Table 2).
|
GROUPS
|
||||||
|
Variables
|
A(n=31)
|
B(n=27)
|
C(n=22)
|
D(n=9)
|
E(n=16)
|
F(n=11)
|
|
Mean ± SD
|
Mean ± SD
|
Mean ± SD
|
Mean ± SD
|
Mean ± SD
|
Mean ± SD
|
|
|
Age (yrs)
|
23.13 ± 4.33
|
42.52 ± 8.71
|
21.68±3.95
|
26.66±3.08
|
42.68±8.61
|
42.27±9.25
|
|
Weight (kg)
|
59.58 ± 10.71
|
63.59 ± 11.31
|
61.22±10.00
|
55.55±11.88
|
68.25±9.90
|
56.81±10.02
|
|
Height (cm)
|
163.87 ± 6.51
|
165.11 ± 10.65
|
165.54±5.40
|
159.77±7.44
|
170±7.88
|
158±10.37
|
|
BSA(m2)
|
1.64 ± 0.17
|
1.40 ± 0.20
|
1.67±0.14
|
1.56±0.18
|
1.78±0.16
|
1.56±0.17
|
|
BMI
|
22.03 ± 2.71
|
23.17 ± 2.50
|
22.22±2.58
|
21.56±3.11
|
23.52±2.28
|
22.65±2.81
|
|
SBP (mm Hg)
|
115.35 ± 11.33
|
121.63 ± 9.69
|
115.90±11.78
|
114±10.67
|
121.5±7.91
|
121.81±12.24
|
|
DBP (mm Hg)
|
74.71 ± 6.19
|
78.89 ± 6.41
|
74.36±5.84
|
75.55±7.26
|
80±6.32
|
77.27±6.46
|
|
Heart Rate (bpm)
|
78.84 ± 13.29
|
82.30 ± 15.87
|
77.09±13.22
|
83.11±13.22
|
79±13.19
|
87.09±18.74
|
Table 2: Demographic Data (n=58)
NS=Not Significant(p>0.05), ** Highly Significant=(p<0 Significant=(p>
Group A: overall subjects (age18-30 years), Group B: overall subjects (age 30-60 years) Group C: Male Subjects (age 18-30yrs),
Group D: Female Subjects-(age 18-30yrs), Group E: Male Subjects-(age 31-60yrs), Group F: Female Subjects-(age 31-60yrs)
|
Variables
|
Study Population (n:58)
|
Male (N-38)
|
Female (N 20)
|
P
|
Age Wise Group (Years)
|
P
|
|||
|
Mean ± SD
|
Mean ± SD
|
P-Val.
|
Sig
|
Group A(Overall)
|
Group B(Overall)
|
P-Val.
|
Sig
|
||
|
(n=31)
|
(n=27)
|
||||||||
|
EPSS (mm)
|
0.60 ± 0.32
|
0.57 ± 0.26
|
0.66 ± 0.41
|
<0.01
|
**
|
0.58 ± 0.37
|
0.63 ± 0.26
|
0.71
|
NS
|
|
Left Atrium (cm)
|
2.80 ± 0.53
|
2.83 ± 0.55
|
2.75 ± 0.49
|
<0.01
|
**
|
2.68 ± 0.40
|
2.94 ± 0.63
|
0.59
|
NS
|
|
IVS d (cm)
|
0.73 ± 0.16
|
0.73 ± 0.17
|
0.73 ± 0.13
|
<0.01
|
**
|
0.70 ± 0.16
|
0.76 ± 0.14
|
0.50
|
NS
|
|
LVID d (cm)
|
4.70 ± 0.47
|
4.84 ± 0.40
|
4.42 ± 0.48
|
<0.01
|
**
|
4.68 ± 0.46
|
4.72 ± 0.48
|
0.07
|
NS
|
|
LVPW d (cm)
|
0.77 ± 0.13
|
0.79 ± 0.13
|
0.73 ± 0.12
|
<0.01
|
**
|
0.73 ± 0.13
|
0.82 ± 0.12
|
0.69
|
NS
|
|
LVEDV (ml)
|
63.38 ± 42.32
|
74.90 ± 43.46
|
41.49 ± 30.40
|
<0.01
|
**
|
79.61 ± 43.10
|
44.75 ± 33.28
|
0.22
|
NS
|
|
LV MASS d (gm)
|
114.40 ± 31.20
|
122.00 ± 29.74
|
99.95 ± 29.37
|
<0.01
|
**
|
108.10 ± 26.82
|
121.63 ± 34.68
|
0.84
|
NS
|
|
CO (L/min)
|
5.43 ± 1.67
|
5.43 ± 1.46
|
5.43 ± 2.07
|
<0.01
|
**
|
5.14 ± 1.37
|
5.75 ± 1.94
|
0.81
|
NS
|
|
E/A RATIO
|
1.41 ± 0.54
|
1.44 ± 0.53
|
1.33 ± 0.56
|
<0.01
|
**
|
1.73 ± 0.48
|
1.03 ± 0.32
|
<0.01
|
**
|
|
Lateral TDI E’
|
6.92 ± 7.34
|
8.38 ± 7.56
|
4.15 ± 6.17
|
<0.01
|
**
|
10.71 ± 7.57
|
2.56 ± 3.90
|
<0.01
|
**
|
|
Lateral TDI E/E’ RATIO
|
0.40 ± 0.40
|
0.32 ± 0.33
|
0.55 ± 0.48
|
0.70
|
NS
|
0.25 ± 0.38
|
0.57 ± 0.35
|
<0.01
|
**
|
|
2D-EF (%)
|
0.65 ± 0.07
|
0.62 ± 0.07
|
0.69 ± 0.06
|
<0.01
|
**
|
0.65 ± 0.07
|
0.64 ± 0.07
|
<0.05
|
*
|
Table 3: Conventional Echocardiogrpahy Data (n=58)
EPSS-Epoint septal separation, IVSd-Inter Ventricular Septum in Diastole, IVPwD-Left Ventricular posterior wall in Diastole, LVID-Left Ventricular, Internal Dimension, LVEDV-Left ventricular end-diastole volume, CO-Cardiac Output, TDI-Tissue Doppler Imaging, EF-Ejection Fraction
NS=Not Significant(p>0.05), ** Highly Significant=(p<0.01), * Significant=(p<0.05) Group A: overall subjects (age18-30 years), Group B: overall subjects (age 30-60 years)
Conventional Echocardiography Data
LA size, E/A ratio, Lateral TDI E’ and Lateral TDI E/E’ ratio are surrogate measurements for assessment of the diastolic function of LV and LVIDd, LVEDV, EPSS and EF% are representative of systolic function. In our study LA size, E/A ratio, lateral TDI E’, LVIDd and LVEDV were significantly higher in males (p<0.01) even though CO & 2D-EF% was higher in females (p<0.01) (Table 3). Additionally, the E/A ratio and 2D-EF% were lower in Group B when compared with Group A (p<0.01), suggesting a reduction in diastolic & systolic function of LV, with increasing age.
4Dimensional Volumetric Data
The sphericity index in diastole and systole, LVEDV, and LVESV were higher in males (p<0.01). Nevertheless, 4D-EF% was more in females (p<0.01) (Table 4). We noticed a decline in sphericity indices in Group B as compared to Group A (p<0.05), suggesting a significant change in LV geometry with increasing age.
M-Mode data of Aortic stiffness
AOS, AOD, Pulsatile change, Pulsatile index, Aortic Strain and Elasticity Modulus were greater in males (p<0.01), and Aortic distensibility was insignificant elevated (p=NS). On the contrary, Aortic Systolic index, Aortic diastolic index was higher in females (p<0.01) (Table 5).
Furthermore, Pulsatile change, Pulsatile index, Aortic Strain were lower in Group B as compared to Group A (P<0.01), demonstrating a decline of these stiffness parameters with increasing age.
|
Variables
|
Study Population (n:58)
|
Male (N-38)
|
Female (N- 20)
|
P
|
Age Wise Group (Years)
|
P
|
|||
|
Mean ± SD
|
Mean ± SD
|
P-Val.
|
Sig
|
Group A(Overall)
|
Group B(Overall)
|
P-Val.
|
Sig
|
||
|
(n=31)
|
(n=27)
|
||||||||
|
EPSS (mm)
|
0.60 ± 0.32
|
0.57 ± 0.26
|
0.66 ± 0.41
|
<0.01
|
**
|
0.58 ± 0.37
|
0.63 ± 0.26
|
0.71
|
NS
|
|
Left Atrium (cm)
|
2.80 ± 0.53
|
2.83 ± 0.55
|
2.75 ± 0.49
|
<0.01
|
**
|
2.68 ± 0.40
|
2.94 ± 0.63
|
0.59
|
NS
|
|
IVS d (cm)
|
0.73 ± 0.16
|
0.73 ± 0.17
|
0.73 ± 0.13
|
<0.01
|
**
|
0.70 ± 0.16
|
0.76 ± 0.14
|
0.50
|
NS
|
|
LVID d (cm)
|
4.70 ± 0.47
|
4.84 ± 0.40
|
4.42 ± 0.48
|
<0.01
|
**
|
4.68 ± 0.46
|
4.72 ± 0.48
|
0.07
|
NS
|
|
LVPW d (cm)
|
0.77 ± 0.13
|
0.79 ± 0.13
|
0.73 ± 0.12
|
<0.01
|
**
|
0.73 ± 0.13
|
0.82 ± 0.12
|
0.69
|
NS
|
|
LVEDV (ml)
|
63.38 ± 42.32
|
74.90 ± 43.46
|
41.49 ± 30.40
|
<0.01
|
**
|
79.61 ± 43.10
|
44.75 ± 33.28
|
0.22
|
NS
|
|
LV MASS d (gm)
|
114.40 ± 31.20
|
122.00 ± 29.74
|
99.95 ± 29.37
|
<0.01
|
**
|
108.10 ± 26.82
|
121.63 ± 34.68
|
0.84
|
NS
|
|
CO (L/min)
|
5.43 ± 1.67
|
5.43 ± 1.46
|
5.43 ± 2.07
|
<0.01
|
**
|
5.14 ± 1.37
|
5.75 ± 1.94
|
0.81
|
NS
|
|
E/A RATIO
|
1.41 ± 0.54
|
1.44 ± 0.53
|
1.33 ± 0.56
|
<0.01
|
**
|
1.73 ± 0.48
|
1.03 ± 0.32
|
<0.01
|
**
|
|
Lateral TDI E’
|
6.92 ± 7.34
|
8.38 ± 7.56
|
4.15 ± 6.17
|
<0.01
|
**
|
10.71 ± 7.57
|
2.56 ± 3.90
|
<0.01
|
**
|
|
Lateral TDI E/E’ RATIO
|
0.40 ± 0.40
|
0.32 ± 0.33
|
0.55 ± 0.48
|
0.70
|
NS
|
0.25 ± 0.38
|
0.57 ± 0.35
|
<0.01
|
**
|
|
2D-EF (%)
|
0.65 ± 0.07
|
0.62 ± 0.07
|
0.69 ± 0.06
|
<0.01
|
**
|
0.65 ± 0.07
|
0.64 ± 0.07
|
<0.05
|
*
|
Table 4: Dimensional volumetric data (n=58
AOS-Aortic dimension in systole, AOD-Aortic dimension in diastole, Ao-Aorta NS=Not Significant(p>0.05), ** Highly Significant=(p<0.01), * Significant=(p<0.05)
Group A: overall subjects (age18-30 years), Group B: overall subjects (age 30-60 years
Tissue Doppler imaging data of Aortic stiffness
SAO, EAO, and AAO were higher in females (p<0.01) (Table 6). It was also observed that EAO was lower in Group B, indicating a deterioration of early diastolicupper wall velocity with aging. Contrarily SAO and AAO showed insignificant (p=NS) increments with increasing age.
|
VARIABLES
|
Study Population (n:58)
|
MALE (N-38)
|
FEMALE (N-20)
|
P
|
Age Wise Group (Years)
|
P
|
|||
|
MEAN ± SD
|
MEAN ± SD
|
P-Val.
|
Sig
|
Group A(Overall)
|
Group B(Overall)
|
P-Val.
|
Sig
|
||
|
(n=31)
|
(n=27)
|
||||||||
|
AOS
|
2.68 ± 0.40
|
2.73 ± 0.38
|
2.59 ± 0.42
|
<0.01
|
**
|
2.53 ± 0.36
|
2.86 ± 0.37
|
0.85
|
NS
|
|
AOD
|
2.22 ± 0.40
|
2.23 ± 0.38
|
2.18 ± 0.45
|
<0.01
|
**
|
2.02 ± 0.33
|
2.44 ± 0.35
|
0.52
|
NS
|
|
Pulsatile Change
|
0.47 ± 0.14
|
0.49 ± 0.14
|
0.42 ± 0.14
|
<0.01
|
**
|
0.51 ± 0.12
|
0.42 ± 0.15
|
<0.01
|
**
|
|
Ao syst. Index
|
1.62 ± 0.26
|
1.59 ± 0.22
|
1.67 ± 0.32
|
<0.01
|
**
|
1.55 ± 0.22
|
1.70 ± 0.27
|
0.59
|
NS
|
|
Ao diast. Index
|
1.34 ± 0.24
|
1.30 ± 0.20
|
1.40 ± 0.31
|
<0.01
|
**
|
1.23 ± 0.19
|
1.45 ± 0.24
|
0.76
|
NS
|
|
Pulsatile Index
|
0.28 ± 0.09
|
0.29 ± 0.09
|
0.27 ± 0.10
|
<0.01
|
**
|
0.31 ± 0.08
|
0.25 ± 0.10
|
<0.01
|
**
|
|
Ao Distensbility (10-6cm2 dyn-1)
|
0.01 ± 0.02
|
0.02 ± 0.03
|
0.01 ± 0.01
|
0.09
|
NS
|
0.02 ± 0.03
|
0.01 ± 0.01
|
0.07
|
NS
|
|
Ao Stiffness Index
|
1.99 ± 0.47
|
1.95 ± 0.38
|
2.08 ± 0.61
|
<0.01
|
**
|
1.76 ± 0.30
|
2.26 ± 0.49
|
0.22
|
NS
|
|
Ao Strain (%) Elasticity
|
22.78 ± 8.86
|
23.58 ± 8.55
|
21.25 ± 9.45
|
<0.01
|
**
|
27.06 ± 7.70
|
17.85 ± 7.51
|
<0.01
|
**
|
|
Elasticity Modulus (Pa)
|
204.16 ± 102.32
|
200.42 ± 80.95
|
211.26 ± 136.27
|
<0.01
|
**
|
159.29 ± 61.37
|
255.67 ± 115.98
|
<0.05
|
*
|
Table 5: Comparison of M-Mode data of Ascending Aorta Data (n=58)
AOS- Aortic dimension in systole, AOD- Aortic dimension in diastole, Ao- Aorta NS=Not Significant(p>0.05), ** Highly Significant=(p<0.01), * Significant=(p<0.05) Group A: overall subjects (age18-30 years), Group B: overall subjects (age 30-60 years
|
Variables
|
Study Population (n:58)
|
Male (N-38)
|
Female (N- 20)
|
P
|
Age Wise Group (Years)
|
P
|
|||
|
Mean ± SD
|
Mean ± SD
|
P-Val.
|
Sig
|
Group A(Overall)
|
Group B(Overall)
|
P-Val.
|
Sig
|
||
|
(n=31)
|
(n=27)
|
||||||||
|
SAO (cm/sec)
|
1.10 ± 0.35
|
1.08 ± 0.35
|
1.14 ± 0.36
|
<0.01
|
**
|
1.06 ± 0.29
|
1.14 ± 0.41
|
0.57
|
NS
|
|
EAO (cm/sec)
|
0.94 ± 0.30
|
0.93 ± 0.32
|
0.96 ± 0.27
|
<0.01
|
**
|
0.98 ± 0.28
|
0.89 ± 0.33
|
<0.05
|
*
|
|
AAO (cm/sec)
|
1.14 ± 0.47
|
1.13 ± 0.44
|
1.15 ± 0.53
|
<0.01
|
**
|
1.07 ± 0.42
|
1.21 ± 0.51
|
0.89
|
NS
|
Table 6: Comparison of TDI data of Ascending Aorta Data (n=58)
TDI-Tissue Doppler imaging, SAO-Systolic upper velocity, EAO-Early diastolic aortic upper wall velocity, AAO-late diastolic upper wall velocity NS=Not Significant(p>0.05), ** Highly Significant=(p<0.01), * Significant=(p<0.05)
Group A: overall subjects (age18-30 years), Group B: overall subjects (age 30-60 years)
Comparison of Aortic stiffness data in various subjects
On comparing Group C and D (male and female subjects of age 18-30 years), it was shown that AOS, AOD, and Aortic Stiffness Index and Elasticity modulus were greater in males of 18-30 years of age (p<0.01), even though Aortic Strain was higher in females (p<0.01) (Table 7). Similarly, SAO, AAO, and EAO reflected a lower value in Group D than Group C, indicating diminished aortic superior wall velocities in female subjects of age 18-30 years of age
|
Variables
|
Groups
|
P
|
Groups
|
P
|
||||
|
C(n=22)
|
D(n=9)
|
P-Value
|
Sig
|
E(n=16)
|
F(n=11)
|
P-Value
|
Sig
|
|
|
Aortic Stiffness Parameters
|
||||||||
|
AOS
|
2.59 ± 0.38
|
2.38 ± 0.26
|
0.000003
|
**
|
2.92 ± 0.29
|
2.77 ± 0.46
|
0.01
|
*
|
|
AOD
|
2.06 ± 0.37
|
1.90 ± 0.20
|
0.000003
|
**
|
2.47 ± 0.25
|
2.41 ± 0.48
|
0.02
|
*
|
|
Ao Distensbility 10-6 cm2 dyn-1)
|
0.02 ± 0.04
|
0.02 ± 0.01
|
0.11
|
NS
|
0.01 ± 0.004
|
0.01 ± 0.01
|
0.62
|
NS
|
|
Ao Stiffness Index
|
1.79 ± 0.31
|
1.67 ± 0.27
|
0.000005
|
**
|
2.16 ± 0.38
|
2.41 ± 0.61
|
0.14
|
NS
|
|
Ao Strain (%)
|
26.77 ± 8.23
|
27.78 ± 6.63
|
0.0001
|
**
|
19.19 ± 7.08
|
15.91 ± 8.04
|
0.01
|
*
|
|
Elasticity Modulus (Pa)
|
167.84 ± 64.25
|
138.40 ± 50.97
|
0.00001
|
**
|
245.22 ± 81.77
|
270.88 ± 156.58
|
0.25
|
NS
|
|
Tissue Doppler Imaging Parameters
|
||||||||
|
SAO (cm/sec)
|
1.10 ± 0.25
|
0.95 ± 0.35
|
0.000003
|
**
|
1.04 ± 0.46
|
1.29 ± 0.30
|
0.44
|
NS
|
|
EAO (cm/sec)
|
1.03 ± 0.28
|
0.88 ± 0.26
|
0.000002
|
**
|
0.79 ± 0.33
|
1.03 ± 0.27
|
0.61
|
NS
|
|
AAO (cm/sec)
|
1.10 ± 0.38
|
0.99 ± 0.54
|
0.00005
|
**
|
1.16 ± 0.53
|
1.29 ± 0.50
|
0.24
|
NS
|
Table 7: Comparison of Aortic Stiffness and Tissue Doppler Imaging data(n=58) Contd
AOS-Aortic dimension in systole, AOD-Aortic dimension in diastole, Ao-Aorta, TDI-Tissue doppler imaging, SAO-Systolic upper velocity, EAO-Early diastolic aortic upper wall velocity, AAO-late diastolic upper wall velocity.
NS=Not Significant(p>0.05), ** Highly Significant=(p<0.01), * Significant=(p<0.05)
Group C: Male Subjects (age 18-30yrs), Group D: Female Subjects-(age 18-30yrs), Group E: Male Subjects-(age 31-60yrs), Group F: Female Subjects-(age 31-60yrs)
|
Variables
|
Groups
|
P
|
Groups
|
P
|
||||
|
C(n=22)
|
D(n=9)
|
P-Value
|
Sig
|
D(n=9)
|
F(n=11)
|
P-Value
|
Sig
|
|
|
Aortic Stiffness Parameters
|
||||||||
|
AOS
|
2.59 ± 0.38
|
2.92 ± 0.29
|
0.14
|
NS
|
2.38 ± 0.26
|
2.77 ± 0.46
|
0.03
|
*
|
|
AOD
|
2.06 ± 0.37
|
2.47 ± 0.25
|
0.30
|
NS
|
1.90 ± 0.20
|
2.41 ± 0.48
|
0.01
|
*
|
|
Ao Distensbility 10-6 cm2 dyn-1)
|
0.02 ± 0.04
|
0.01 ± 0.004
|
0.10
|
NS
|
0.02 ± 0.01
|
0.01 ± 0.01
|
0.58
|
NS
|
|
Ao Stiffness Index
|
1.79 ± 0.31
|
2.16 ± 0.38
|
0.34
|
NS
|
1.67 ± 0.27
|
2.41 ± 0.61
|
0.002
|
**
|
|
Ao Strain (%)
|
26.77 ± 8.23
|
19.19 ± 7.08
|
0.0001
|
**
|
27.78 ± 6.63
|
15.91 ± 8.04
|
0.15
|
NS
|
|
Elasticity Modulus (Pa)
|
167.84 ± 64.25
|
245.22 ± 81.77
|
0.74
|
NS
|
138.40 ± 50.97
|
270.88 ± 156.58
|
0.01
|
*
|
|
Tissue Doppler Imaging Parameters
|
||||||||
|
SAO (cm/sec)
|
1.10 ± 0.25
|
1.04 ± 0.46
|
0.02
|
*
|
0.95 ± 0.35
|
1.29 ± 0.30
|
0.01
|
*
|
|
EAO (cm/sec)
|
1.03 ± 0.28
|
0.79 ± 0.33
|
0.0004
|
**
|
0.88 ± 0.26
|
1.03 ± 0.27
|
0.05
|
*
|
|
AAO (cm/sec)
|
1.10 ± 0.38
|
1.16 ± 0.53
|
0.13
|
NS
|
0.99 ± 0.54
|
1.29 ± 0.50
|
0.07
|
NS
|
Table 8: Comparison of Aortic Stiffness and Tissue Doppler Imaging data (n=58) Contd
AOS-Aortic dimension in systole, AOD-Aortic dimension in diastole, Ao-Aorta, TDI-Tissue doppler imaging, SAO-Systolic upper velocity, EAO-Early diastolic aortic upper wall velocity, AAO-late diastolic upper wall velocity.
NS=Not Significant(p>0.05), ** Highly Significant=(p<0.01), * Significant=(p<0.05)
Group C: Male Subjects (age 18-30yrs), Group D: Female Subjects-(age 18-30yrs), Group E: Male Subjects-(age 31-60yrs), Group F: Female Subjects-(age 31-60yrs)
In addition, when we analyzed the data of Group E and F (male and female subjects of age 31-60 years), it was noted that AOS, AOD, and Aortic strain values were higher in Group E than in Group F. Conversely, the SAO, AAO, and EAO values were more in Group F, even though insignificantly (p=NS).
Interestingly, only Aortic strain was lower in Group E when compared to Group C (P<0.01), implying that aortic strain was deteriorating with increasing age in male subjects (Table 8). On the contrary, AOS, AOD, Aortic stiffness index, and Elasticity modulus were insignificantly higher in Group E (p=NS). We also observed that SAO values were higher and EAO values were lower in Group E (p<0.01), on comparing with Group C.
Subsequently, on collating the Aortic stiffness data in female subjects (Group D and F) we found higher values of AOS, AOD, Aortic Stiffness Index, and Elasticity modulus in Group F than in D (p<0.05, p<0.05, p<0.01, p<0.05), suggesting that in female adults that there is a decline in these stiffness parameters with advancing age. Simultaneously SAO and EAO were also higher in Group F (p<0.05).
We have extensively estimated the Age and Gender- specific values of Aortic Stiffness in various subsets of our study population. Here we are furnishing a summarized value (Table 9) of the above-mentioned parameters discerned from the current study. This table is particularly meant for contemporary and prospective medical researchers to conceptualize further these interesting original findings
|
Variables
|
Study Population (n:58)
|
Male
(n-38)
|
Female
(n-20)
|
GROUPS
|
|||||
|
Mean ± SD
|
Mean ± SD
|
A(n=31)
|
B(n=27)
|
C(n=22)
|
D(n=9)
|
E(n=16)
|
F(n=11)
|
||
|
Mean ± SD
|
Mean ± SD
|
Mean ± SD
|
Mean ± SD
|
Mean ± SD
|
Mean ± SD
|
||||
|
M-mode parameter
|
|||||||||
|
Ao Distensbility (10-6 cm2 dyn-1)
|
0.01 ± 0.02
|
0.02 ± 0.03
|
0.01 ± 0.01
|
0.02 ± 0.03
|
0.01 ± 0.01
|
0.02 ± 0.04
|
0.02 ± 0.01
|
0.01 ± 0.004
|
0.01 ± 0.01
|
|
Ao Stiffness Index
|
1.99 ± 0.47
|
1.95 ± 0.38
|
2.08 ± 0.61
|
1.76 ± 0.30
|
2.26 ± 0.49
|
1.79 ± 0.31
|
1.67 ± 0.27
|
2.16 ± 0.38
|
2.41 ± 0.61
|
|
Ao Strain (%)
|
22.78 ± 8.86
|
23.58 ± 8.55
|
21.25 ± 9.45
|
27.06 ± 7.70
|
17.85 ± 7.51
|
26.77 ± 8.23
|
27.78 ± 6.63
|
19.19 ± 7.08
|
15.91 ± 8.04
|
|
Elasticity Modulus (Pa)
|
204.16 ± 102.32
|
200.42 ± 80.95
|
211.26 ± 136.27
|
159.29 ± 61.37
|
255.67 ± 115.98
|
167.84 ± 64.25
|
138.40 ± 50.97
|
245.22 ± 81.77
|
270.88 ± 156.58
|
|
Tissue Doppler Imaging Parameters
|
|||||||||
|
SAO (cm/sec)
|
1.10 ± 0.35
|
1.08 ± 0.35
|
1.14 ± 0.36
|
1.06 ± 0.29
|
1.14 ± 0.41
|
1.10 ± 0.25
|
0.95 ± 0.35
|
1.04 ± 0.46
|
1.29 ± 0.30
|
|
EAO (cm/sec)
|
0.94 ± 0.30
|
0.93 ± 0.32
|
0.96 ± 0.27
|
0.98 ± 0.28
|
0.89 ± 0.33
|
1.03 ± 0.28
|
0.88 ± 0.26
|
0.79 ± 0.33
|
1.03 ± 0.27
|
|
AAO (cm/sec)
|
1.14 ± 0.47
|
1.13 ± 0.44
|
1.15 ± 0.53
|
1.07 ± 0.42
|
1.21 ± 0.51
|
1.10 ± 0.38
|
0.99 ± 0.54
|
1.16 ± 0.53
|
1.29 ± 0.50
|
Table 9: Summary of Aortic Stiffness Parameter
NB: All values in the above table are MEAN ± SD
SAO- Systolic upper velocity, EAO- Early diastolic aortic upper wall velocity, AAO-late diastolic upper wall velocity, Ao-Aortic Group A: overall subjects (age18-30 years), Group B: overall subjects (age 30-60 years) Group C: Male Subjects (age 18-30yrs), Group D: Female Subjects-(age 18-30yrs), Group E: Male Subjects-(age 31-60yrs), Group F: Female Subjects-(age 31-60yrs)
Discussion
It is well known that increased aortic stiffness has been associated with impaired LV systolic and diastolic functions. The association between increased stiffness and LV systolic dysfunction, has been demonstrated in a previous study [34], particularly along the long axis. The relation is often attributed to increased hemodynamic load caused by stiffer arteries [35,36]. An alternative explanation for the observed relation between aortic stiffness and LV systolic function, is the direct mechanical ventricular-vascular coupling.
Systolic contraction shortens the LV long axis by pulling the aortic annulus and sino-tubular junction of the aorta towards the LV apex, which moves minimally during systole [37-40]. The combination of aortic annulus displacement along with sparse movement of the aortic arch implies that there is substantial longitudinal stretch of the ascending aorta during systole [40-42].
Abhayaratna et al [43] assessed the relationship of arterial stiffness with LV diastolic dysfunction in 188 elderly individuals and found a significant correlation between central pulse pressure and severity of diastolic dysfunction and concluded that increased arterial stiffness was associated with more severe left ventricular diastolic dysfunction.
Arterial stiffness index establishes the elastic properties of the arterial wall, in a manner relatively independent of blood pressure, and aortic distensibility evaluates the ability of the arteries to dilate during the cardiac cycle [44-51].
Aortic stiffness and aortic distensibility have been examined with VVI and pulse wave velocity (PWV) [46,52]. However, VVI is a new and invasive method, requiring transesophageal echocardiography, which limits its routine use in clinical practice. Also, PWV is not the ideal procedure to evaluate aortic elasticity properties since it is affected by many factors including hematological and physiological characteristics, as well as heart rate and blood pressure variations [53-55].
Direct measurements of aortic elasticity by TDI, which is a practical method for the measurements of diameter changes related to wall movements, may provide further help than other methods described above, because it is not affected by hematological and cardiovascular physiology [56-58]. Multiple articles have shown a link between loss of elasticity in major arteries and cardiovascular adverse events [57,58]. In the Framingham Cardiology study, over 20 years of monitoring, increased pulse pressure, which is an indication of large vessel wall stiffness has been shown to increase coronary artery disease risk in the middle and older age group, who had no clinical coronary artery disease [59].
Hence the, determination of normal value ranges of Aortic stiffness parameters is imperative, because then only the normal values can be compared to the values obtained in different disease states.
A considerable amount of literature is available on the adverse impact caused by various disease states on the aortic stiffness parameters, nevertheless, it is exceptionally rare to find a study depicting these values in healthy population. After a deep search of the literature, we could only come across a solitary study [25] which has recently endeavoured to put forward the normal values ranges of Aortic stiffness properties in healthy population by 2Dimensional and 4Dimensional XStrain Echocardiography. There were 72 healthy participants in the 2Dimensional group and 30 individuals in the 4D XStrain group. The results are analogous to the current study, even though there were small number of subjects in 4D XStrain group.
In the study of elasticity properties of ascending aorta in healthy children and adolescents [60] 165 subjects were enrolled with a mean age of 11.92±4.0 years. The mean age in our study group was 32.16±11.82 years and to compare their data with the present study would not be feasible. Another research study investigated the effects of subclinical hypothyroidism on elastic properties of the ascending [17]. This study had a strict inclusion criterion and they recruited 48 healthy controls with a mean age of 42±11 years. The values of their control group are incongruous with our study and the reason seems to be the disparity of mean age of the controls of their study and the healthy subjects of the present study. Correspondingly Vitarelli et al [14] reported in their 80 healthy controls, two-dimensional M-mode and TDI guided ascending aorta wall stiffness parameters. The mean age was 49±17 years and the values of stiffness index (SI), Aortic distensibility (D), elastic modulus (EM), SEO, AAO and EAO reflected gross incongruity with our study group. The divergence of results may be because of dissimilarities in the mean age of our study group and their control group (mean age 49 ±17 years)
Gungor et al [15] showed that aortic stiffness is increased in patients with premature coronary artery disease (CAD). In their study there were 50 patients of acute coronary (ACS) and 70 age sex matched controls. However, in their control groups there were 26 smokers and several were having hypertension, diabetes and hyperlipidemia controlled on medication. Nevertheless, the mean age in their study group was 34±3.9 years which is similar to our study. Since this study included, in their control group volunteers who were current smokers, controlled hypertensives, diabetics and hyperlipidemics therefore to collate the results of aortic stiffness in their control group with our study would not be meaningful.
Earlier studies mentioned above are in some way or the other, inharmonious with the present research work. We have extensively compared our data in healthy population by constructing various subsets of groups and then collating the values amongst them, in a judicious manner. The main results of our study can be outlined as follows: (i) we provided exhaustive data on several parameters of Aortic stiffness determined by M-mode and TDI echocardiography. (ii) Our study group was arbitrarily divided into six groups A-E (iii) 4Dimensional volumetric data : sphericity index, LVEDV and LVESV were higher in males and importantly, 4D-EF was more in females (iv) AOS, AOD, Aortic strain, and elasticity modulus were greater in males (v) On the contrary Aortic superior wall velocities (SAO, EAO, AAO) were higher in females (vi) Increasing age lead to a decline in parameters of sphericity index, and majority of stiffness parameters derived by M-mode echocardiography (vii) correspondingly EAO determined by TDI of superior wall of aorta, showed a deterioration with advancing age.
Study Limitations
The echocardiographic method of determining the aortic stiffness using mathematical equations may have some limitations [56,57]. Firstly, blood pressure and pulse pressure measured at the level of the brachial artery may not exactly reflect aortic pulse pressure, and secondly, blood pressure measurement and aortic echocardiographic assessment cannot be carried out simultaneously. All the participants are of Indian ethnicity and the normal value ranges of the present study cannot be anticipated to be identical with other ethnic groups, particularly Caucasians.
Our study had a modest number of subjects because it was undertaken during the raging corona pandemic and to encounter a normal healthy subject during this period was an arduous task. Moreover, this is a single-center experience.
Recommendations and future research directions
The authors recommend, in the future large-scale multiple-center randomized controlled trials for enrolling hundreds of healthy subjects to further investigate the important properties of Aortic stiffness.
Conclusion
The authors report a normal range of M-mode and TDI- derived values of Aortic stiffness of ascending aorta, in healthy Indian adults. The difference in magnitude of aortic elasticity indices has been demonstrated in men and women, as well as in different subsets of the study group.
Conflict of Interest
The authors declare no conflict of interests.
References
- Vizzardi, Enrico, Giorgio Caretta, Ivano Bonadei, Riccardo Rovetta, Edoardo Sciatti, Natalia Pezzali, Carlo M. Lombardi et al. "Echocardiographic elastic properties of ascending aorta and their relationship with exercise capacity in patients with non-ischemic dilated cardiomyopathy." IJC Heart & Vessels 3 (2014): 78-81.
- Malayeri, Ashkan A., Shunsuke Natori, Hossein Bahrami, Alain G. Bertoni, Richard Kronmal, João AC Lima, and David A. Bluemke. "Relation of aortic wall thickness and distensibility to cardiovascular risk factors (from the Multi-Ethnic Study of Atherosclerosis [MESA])." The American journal of cardiology 102, no. 4 (2008): 491-496.
- O’rourke, Michael F., and Junichiro Hashimoto. "Mechanical factors in arterial aging: a clinical perspective." Journal of the American College of Cardiology 50, no. 1 (2007): 1-13.
- Malayeri, Ashkan A., Shunsuke Natori, Hossein Bahrami, Alain G. Bertoni, Richard Kronmal, João AC Lima, and David A. Bluemke. "Relation of aortic wall thickness and distensibility to cardiovascular risk factors (from the Multi-Ethnic Study of Atherosclerosis [MESA])." The American journal of cardiology 102, no. 4 (2008): 491-496.
- Stefanadis, Christodoulos, Costas Stratos, Charalambos Vlachopoulos, Stelios Marakas, Harisios Boudoulas, Ioannis Kallikazaros, Eleftherios Tsiamis, Konstantinos Toutouzas, Lambros Sioros, and Pavlos Toutouzas. "Pressure-diameter relation of the human aorta: a new method of determination by the application of a special ultrasonic dimension catheter." Circulation 92, no. 8 (1995): 2210-2219.
- Chen, Chen-Huan, Chih-Tai Ting, Amit Nussbacher, Erez Nevo, David A. Kass, Peter Pak, Shih-Pu Wang, Mau-Song Chang, and Frank CP Yin. "Validation of carotid artery tonometry as a means of estimating augmentation index of ascending aortic pressure." Hypertension 27, no. 2 (1996): 168-175.
- Kim, Kye Hun, Jong Chun Park, Hyun Ju Yoon, Nam Sik Yoon, Young Joon Hong, Hyung Wook Park, Ju Han Kim et al. "Usefulness of aortic strain analysis by velocity vector imaging as a new echocardiographic measure of arterial stiffness." Journal of the American Society of Echocardiography 22, no. 12 (2009): 1382-1388.
- Shimojo, Michio, Nobuyuki Tsuda, Toshiji Iwasaka, and Mitsuo Inada. "Age-related changes in aortic elasticity determined by gated radionuclide angiography in patients with systemic hypertension or healed myocardial infarcts and in normal subjects." The American journal of cardiology 68, no. 9 (1991): 950-953.
- Gregory, Alexander, Marelise Kruger, Neal Maher, Randy Moore, and Gary Dobson. "Non-invasive determination of aortic mechanical properties and their effects on left ventricular function following endovascular abdominal aneurysm repair." Journal of Medical and Biological Engineering 39 (2019): 739- 751.
- Karamitsos, T. D., H. I. Karvounis, T. P. Didangellos, C. E. Papadopoulos, E. G. Dalamanga, D. T. Karamitsos, G. E. Parharidis, and G. E. Louridas. "Usefulness of colour tissue Doppler imaging in assessing aortic elastic properties in Type 1 diabetic patients." Diabetic medicine 23, no. 11 (2006): 1201-1206.
- Özhan, Hakan, Mehmet Yazici, Sinan Albayrak, Enver Erbilen, Serkan Bulur, Ramazan Akdemir, and Cihangir Uyan. "Elastic properties of the ascending aorta and left ventricular function in patients with hypothyroidism." Echocardiography: A Journal of Cardiovascular Ultrasound and Allied Techniques 22, no. 8 (2005): 649-656.
- Harada, Kenji, Kenji Yasuoka, and Yoichi Shimada. "Usefulness of tissue doppler imaging for assessing aortic wall stiffness in children with the Marfan syndrome." The American journal of cardiology 93, no. 8 (2004): 1072-1075.
- Schmidt-Trucksäss, Arno, Dominik Grathwohl, Andreas Schmid, Raffael Boragk, Christine Upmeier, Joseph Keul, and Martin Huonker. "Assessment of carotid wall motion and stiffness with tissue Doppler imaging." Ultrasound in medicine & biology 24, no. 5 (1998): 639-646.
- Vitarelli, Antonio, Marcello Giordano, Giuseppe Germanò, Mario Pergolini, Paolo Cicconetti, Francesco Tomei, Angela Sancini et al. "Assessment of ascending aorta wall stiffness in hypertensive patients by tissue Doppler imaging and strain Doppler echocardiography." Heart 96, no. 18 (2010): 1469- 1474.
- Güngör, Barış, Hale Yılmaz, Ahmet Ekmekçi, Kazım Serhan Özcan, Mohamedou Tijani, Damirbek Osmonov, Baran Karataş et al. "Aortic stiffness is increased in patients with premature coronary artery disease: a tissue Doppler imaging study." Journal of cardiology 63, no. 3 (2014): 223-229.
- Vizzardi, Enrico, Edoardo Sciatti, Ivano Bonadei, Elisa Menotti, Francesco Prati, Marta Scodro, Lucia Dallapellegrina et al. "Elastic aortic properties in cystic fibrosis adults without cardiovascular risk factors: A case-control study." Echocardiography 36, no. 6 (2019): 1118-1122.
- Yurtdaş, Mustafa, Ramazan Gen, Turkay Özcan, and Mehmet Kasım Aydın. "Assessment of the elasticity properties of the ascending aorta in patients with subclinical hypothyroidism by tissue Doppler imaging." Arquivos Brasileiros de Endocrinologia & Metabologia 57 (2013): 132-138.
- Ardic, Idris, Mikail Yarlioglues, Orhan Dogdu, Hakan Buyukoglan, Asiye Kanbay, Mahmut Akpek, Canan Bol et al. "Assessment of aortic elastic properties in patients with sarcoidosis." Blood pressure 21, no. 5 (2012): 286-292.
- Vizzardi, Enrico, Luciano Corda, Natalia Pezzali, Elisa Roca, Laura Pini, Antonio D'Aloia, Marco Metra, Livio Dei Cas, and Claudio Tantucci. "Elastic properties of the ascending aorta in patients with α1-antitrypsin deficiency (Z homozygotes)." Heart 98, no. 18 (2012): 1354-1358.
- Kaya, Cevdet, Mehmet Ergelen, Abdullah Ilktac, and M. Ihsan Karaman. "Impaired elasticity of aorta in patients with erectile dysfunction." Urology 70, no. 3 (2007): 558-562.
- Kasikcioglu, Hulya Akhan, Levent Karasulu, Ebru Durgun, Huseyin Oflaz, Erdem Kasikcioglu, and Caglar Cuhadaroglu. "Aortic elastic properties and left ventricular diastolic dysfunction in patients with obstructive sleep apnea." Heart and vessels 20 (2005): 239-244.
- Vizzardi, Enrico, Eleftheria Trichaki, Ivano Bonadei, Edoardo Sciatti, Francesca Salghetti, Riccardo Raddino, and Marco Metra. "Elastic aortic properties in patients with X syndrome." Heart, Lung and Circulation 23, no. 2 (2014): 114-118.
- Kardesoglu, Ejder, Namik Ozmen, Mustafa Aparci, Bekir Sitki Cebeci, Omer Uz, and Mehmet Dincturk. "Abnormal elastic properties of the aorta in the mitral valve prolapse syndrome." Acta cardiologica 62, no. 2 (2007): 151-155.
- Seyfeli, E., M. Duru, H. Saglam, F. Akgul, G. Kuvandik, H. Kaya, and F. Yalcin. "Association of left ventricular diastolic function abnormalities with aortic elastic properties in asymptomatic patients with type 2 diabetes mellitus. A tissue doppler echocardiographic study." International journal of clinical practice 62, no. 9 (2008): 1358-1365.
- Mehrotra, Akhil, Ajay Sharma, Mohammad Shadab, Mukesh Srivastava, Naveen Chandra, and A. Singh. "Dimensional X strain and 2Dimensional speckle tracking echocardiographic study: normative values of strain parameters of left ventricle and tissue doppler imaging of ascending aorta in healthy adults-a Single Centre Indian Study." Texila Int J Acad Res 9 (2022): 120-41.
- Mehrotra, Akhil, Ajay Sharma, Mohammad Shadab, Om Prakash, and Shubham Kacker. "Four-Dimensional XStrain Echocardiography: Correlation of Aortic Stiffness with Left Ventricular Diastolic, Systolic, and Strain Parameters in Healthy Adults–A Single-center Indian Perspective." Journal of Indian College of Cardiology 13, no. 1 (2023): 29-39.
- Lehmann, E. D. "Noninvasive measurements of aortic stiffness: methodological considerations." Pathologie-biologie 47, no. 7 (1999): 716-730.
- Benetos, Athanase, Stephane Laurent, A. P. Hoeks, P. H. Boutouyrie, and M. E. Safar. "Arterial alterations with aging and high blood pressure. A noninvasive study of carotid and femoral arteries." Arteriosclerosis and thrombosis: a journal of vascular biology 13, no. 1 (1993): 90-97.
- Muraru, Denisa, Alice Niero, Hugo Rodriguez-Zanella, Diana Cherata, and Luigi Badano. "Three-dimensional speckle-tracking echocardiography: benefits and limitations of integrating myocardial mechanics with three-dimensional imaging." Cardiovascular diagnosis and therapy 8, no. 1 (2018): 101.
- Lang, Roberto M., Luigi P. Badano, Victor Mor-Avi, Jonathan Afilalo, Anderson Armstrong, Laura Ernande, Frank A. Flachskampf et al. "Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging." European Heart Journal- Cardiovascular Imaging 16, no. 3 (2015): 233-271.
- Voigt, J. U., Pedrizzetti, G., Lysyansky, P., Marwick, T. H., Houle, H., Baumann, R., Pedri, S., Ito, Y., Abe, Y., Metz, S., Song, J. H., Hamilton, J., Sengupta, P. P., Kolias, T. J., d'Hooge, J., Aurigemma, G. P., Thomas, J. D., & Badano, L. P. (2015). Definitions for a common standard for 2D speckle tracking echocardiography: consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography, 28(2), 183–193.
- Di Bella, G., S. Pedri, and M. Schreckenberg. "Three and four dimensional quantification of left ventricular volumes and ejection fraction on the basis of feature strain echocardiography." G Ital Cardiol 106 (2011): 12.
- Dragulescu, Andrea, Lars Grosse-Wortmann, Cheryl Fackoury, and Luc Mertens. "Echocardiographic assessment of right ventricular volumes: a comparison of different techniques in children after surgical repair of tetralogy of Fallot." European Heart Journal–Cardiovascular Imaging 13, no. 7 (2012): 596-604.
- Bell, Vanessa, Elizabeth L. McCabe, Martin G. Larson, Jian Rong, Allison A. Merz, Ewa Osypiuk, Birgitta T. Lehman et al. "Relations between aortic stiffness and left ventricular mechanical function in the community." Journal of the American Heart Association 6, no. 1 (2017): e004903.
- Kim, Hack-Lyoung, Jae-Bin Seo, Woo-Young Chung, Sang- Hyun Kim, Myung-A. Kim, and Joo-Hee Zo. "Independent association between brachial-ankle pulse wave velocity and global longitudinal strain of left ventricle." The International Journal of Cardiovascular Imaging 31 (2015): 1563-1570.
- Krishnasamy, Rathika, Carmel M. Hawley, Tony Stanton, Elaine M. Pascoe, Katrina L. Campbell, Megan Rossi, William Petchey et al. "Left ventricular global longitudinal strain is associated with cardiovascular risk factors and arterial stiffness in chronic kidney disease." BMC nephrology 16 (2015): 1-9.
- Beller, Carsten J., Michel R. Labrosse, Mano J. Thubrikar, and Francis Robicsek. "Role of aortic root motion in the pathogenesis of aortic dissection." Circulation 109, no. 6 (2004): 763-769.
- Kozerke, Sebastian, Markus B. Scheidegger, Erik M. Pedersen, and Peter Boesiger. "Heart motion adapted cine phase-contrast flow measurements through the aortic valve." Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine 42, no. 5 (1999): 970-978.
- Bell, Vanessa, William A. Mitchell, Sigurður Sigurðsson, Jos JM Westenberg, John D. Gotal, Alyssa A. Torjesen, Thor Aspelund et al. "Longitudinal and circumferential strain of the proximal aorta." Journal of the American Heart Association 3, no. 6 (2014): e001536.
- Weber, Tim F., Tobias Müller, Andreas Biesdorf, Stefan Wörz, Fabian Rengier, Tobias Heye, Tim Holland-Letz, Karl Rohr, Hans-Ulrich Kauczor, and Hendrik von Tengg-Kobligk. "True four-dimensional analysis of thoracic aortic displacement and distension using model-based segmentation of computed tomography angiography." The international journal of cardiovascular imaging 30 (2014): 185-194.
- Morrison, Tina M., Gilwoo Choi, Christopher K. Zarins, and Charles A. Taylor. "Circumferential and longitudinal cyclic strain of the human thoracic aorta: age-related changes." Journal of vascular surgery 49, no. 4 (2009): 1029-1036.
- Bell, Vanessa, Sigurdur Sigurdsson, Jos JM Westenberg, John D. Gotal, Alyssa A. Torjesen, Thor Aspelund, Lenore J. Launer et al. "Relations between aortic stiffness and left ventricular structure and function in older participants in the Age, Gene/ Environment Susceptibility-Reykjavik Study." Circulation: Cardiovascular Imaging 8, no. 4 (2015): e003039.
- Abhayaratna, Walter P., Marion E. Barnes, Michael F. O’Rourke, Bernard J. Gersh, James B. Seward, Yoko Miyasaka, Kent R. Bailey, and Teresa SM Tsang. "Relation of arterial stiffness to left ventricular diastolic function and cardiovascular risk prediction in patients≥ 65 years of age." The American journal of cardiology 98, no. 10 (2006): 1387-1392.
- Wagenseil, Jessica E., and Robert P. Mecham. "Vascular extracellular matrix and arterial mechanics." Physiological reviews 89, no. 3 (2009): 957-989.
- McEniery, Carmel M., Ian B. Wilkinson, and Albert P. Avolio. "Age, hypertension and arterial function." Clinical and Experimental Pharmacology and Physiology 34, no. 7 (2007): 665- 671.
- Kim, Kye Hun, Jong Chun Park, Hyun Ju Yoon, Nam Sik Yoon, Young Joon Hong, Hyung Wook Park, Ju Han Kim et al. "Usefulness of aortic strain analysis by velocity vector imaging as a new echocardiographic measure of arterial stiffness." Journal of the American Society of Echocardiography 22, no. 12 (2009): 1382-1388.
- Eryol, Namik Kemal, Ramazan Topsakal, Yüksel Çiçek, Adnan Abaci, Abdurahman Oguzhan, Emrullah Basar, and Ali Ergin. "Color Doppler tissue imaging in assessing the elastic properties of the aorta and in predicting coronary artery disease." Japanese heart journal 43, no. 3 (2002): 219-230.
- Karamitsos, T. D., H. I. Karvounis, T. P. Didangellos, C. E. Papadopoulos, E. G. Dalamanga, D. T. Karamitsos, G. E. Parharidis, and G. E. Louridas. "Usefulness of colour tissue Doppler imaging in assessing aortic elastic properties in Type 1 diabetic patients." Diabetic medicine 23, no. 11 (2006): 1201-1206.
- Vitarelli, Antonio, Marcello Giordano, Giuseppe Germanò, Mario Pergolini, Paolo Cicconetti, Francesco Tomei, Angela Sancini et al. "Assessment of ascending aorta wall stiffness in hypertensive patients by tissue Doppler imaging and strain Doppler echocardiography." Heart 96, no. 18 (2010): 1469- 1474.
- Özhan, Hakan, Mehmet Yazici, Sinan Albayrak, Enver Erbilen, Serkan Bulur, Ramazan Akdemir, and Cihangir Uyan. "Elastic properties of the ascending aorta and left ventricular function in patients with hypothyroidism." Echocardiography: A Journal of Cardiovascular Ultrasound and Allied Techniques 22, no. 8 (2005): 649-656.
- Korpas, David, and Jan Halek. "Pulse wave variability within two short-term measurements." Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 150, no. 2 (2006): 339-344.
- 52 Asmar, R., Benetos, A., Topouchian, J., Laurent, P., Pannier, B., Brisac, A. M., ... & Levy, B. I. (1995). Assessment of arterial distensibility by automatic pulse wave velocity measurement: validation and clinical application studies. Hypertension, 26(3), 485-490.
- Bia, Daniel, Ismael Aguirre, Yanina Zócalo, Lucía Devera, Edmundo Cabrera Fischer, and Ricardo Armentano. "Regional differences in viscosity, elasticity, and wall buffering function in systemic arteries: pulse wave analysis of the arterial pressure- diameter relationship." Revista Española de Cardiología (English Edition) 58, no. 2 (2005): 167-174.
- Lehmann, E. D. "Noninvasive measurements of aortic stiffness: methodological considerations." Pathologie-biologie 47, no. 7 (1999): 716-730.
- Lantelme, Pierre, Christine Mestre, Michel Lievre, Alain Gressard, and Hugues Milon. "Heart rate: an important confounder of pulse wave velocity assessment." Hypertension 39, no. 6 (2002): 1083-1087.
- Benetos, Athanase, Stephane Laurent, A. P. Hoeks, P. H. Boutouyrie, and M. E. Safar. "Arterial alterations with aging and high blood pressure. A noninvasive study of carotid and femoral arteries." Arteriosclerosis and thrombosis: a journal of vascular biology 13, no. 1 (1993): 90-97.
- O’Rourke, Michael, and Edward D. Frohlich. "Pulse pressure: is this a clinically useful risk factor?." Hypertension 34, no. 3 (1999): 372-374.
- Feistritzer, Hans-Josef, Gert Klug, Sebastian J. Reinstadler, Martin Reindl, Lea Niess, Timo Nalbach, Christian Kremser, Agnes Mayr, and Bernhard Metzler. "Prognostic value of aortic stiffness in patients after ST-elevation myocardial infarction." Journal of the American Heart Association 6, no. 9 (2017): e005590.
- Nakanishi, Noriyuki, Kenji Suzuki, and Kozo Tatara. "Clustered features of the metabolic syndrome and the risk for increased aortic pulse wave velocity in middle-aged Japanese men." Angiology 54, no. 5 (2003): 551-559.
- Hauser, Michael, Andreas Kühn, Kurt Petzuch, Petra Wolf, and Manfred Vogt. "Elastic Properties of the Ascending Aorta in Healthy Children and Adolescents–Age-Related Reference Values for Aortic Wall Stiffness and Distensibility Obtained on M-mode Echocardiography–." Circulation Journal 77, no. 12 (2013): 3007-3014.


