
Case Report | DOI: https://doi.org/10.58489/2836-5062/012
*Corresponding Author: Dr. Sachin s kadam
Citation: Dr. Sachin s kadam. Synchronus Oral Squamous Cell Carcinoma in A Female: A Rare Case Report. Journal of Clinical Oncology Reports.2(3). DOI:10.58489/2836-5062/012
Copyright: © Dr. Sachin s kadam, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 February 2023 | Accepted: 12 April 2023 | Published: 14 April 2023
Keywords: Synchronus, Oral Squamous, Cell Carcinoma ,more aggressive, more resistant
Worldwide, the number of new cases of lip and oral cavity cancer in both sexes, all age groups in 2020 are around 377713 and the number of deaths in both sexes, all age groups are around 177757. In India, lip and oral cavity cancer ranks at 2nd position with incidence around 10.3%, mortality 8.8% and 5- year prevalence around21.77%. Multiple theories have been put forth describing the multifocal origin of squamous cell carcinoma (SCC) of the oral and aerodigestive tract. “Field Cancerization “is the first theory described in oral squamous cell carcinoma (SCC) which explains the multifocal or synchronous origin of the SCC. Synchronous carcinomas are defined as second neoplasms at the same time or within 6 months period of primary lesions. After that, they are described as metachronous neoplasms. The criteria to describe synchronous tumours were elaborated by Warren and Gates and Moertel et al. “Field Cancerization “theory was explained by widespread epithelial exposure to carcinogens; however, the alternative theory of common clonal origin is now supported by the recent molecular studies. Second Primary Tumours (Synchronous or Metachronous) are usually more aggressive, more resistant, metastasizes early and they require a more aggressive treatment strategy. Hence, their early detection is the crucial step in planning the best possible management. We are reporting an unusual case of synchronous oral squamous cell carcinoma in 58-year-old female who underwent surgery followed by adjuvant treatment after diagnosis.
Worldwide, the number of new cases of lip and oral cavity cancer in both sexes, all age groups in 2020 are around 377713 and the number of deaths in both sexes, all age groups are around 177757 [ 1]. In India, lip and oral cavity cancer ranks at 2nd position with incidence around 10.3%, mortality 8.8% and 5- year prevalence around21.77% [ 2]. Multiple theories have been put forth describing the multifocal origin of squamous cell carcinoma (SCC) of the oral and aerodigestive tract [ 3]. “Field Cancerization “is the first theory described in oral squamous cell carcinoma (SCC) which explains the multifocal or synchronous origin of the SCC [ 4]. Synchronous carcinomas are defined as second neoplasms at the same time or within 6 months period of primary lesions. After that, they are described as metachronous neoplasms. [ 5]. The criteria to describe synchronous tumours were elaborated by Warren and Gates and Moertel et al [ 6]. “Field Cancerization “theory was explained by widespread epithelial exposure to carcinogens; however, the alternative theory of common clonal origin is now supported by the recent molecular studies [ 7]. Second Primary Tumours (Synchronous or Metachronous) are usually more aggressive, more resistant, metastasizes early and they require a more aggressive treatment strategy. Hence, their early detection is the crucial step in planning the best possible management [ 8]. We are reporting an unusual case of synchronous oral squamous cell carcinoma in 58-year-old female who underwent surgery followed by adjuvant treatment after diagnosis.
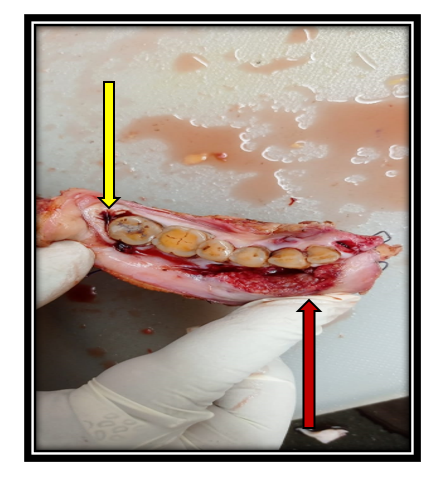
A 58year old lady with Eastern Co-operative Oncology Group Performance Status 1 (ECOG PS-1) presented to our clinic. She had history of ulcerative lesion at right lower alveolus for the last 2 months. She was receiving treatment for diabetes mellitus and hypertension. There was no contributory family, past and surgical history. She had history of tobacco chewing for the last 25 years in the form of ‘Pan ‘. On clinical examination, there were two lesions in the oral cavity. One lesion was located at right lower gingivo-buccal sulcus of size 2.5x 1cm in relation to canine tooth and second lesion was located at right retromolar triagone with size 1.5 x 1cm. Right level IB lymph node was enlarged. Punch biopsy was already taken by the treating physician and it was reported as moderately differentiated squamous cell carcinoma. Rest of the systemic examination was unremarkable. She had been advised CECT of oral cavity, neck and chest. CECT was suggestive of same findings with no distant metastasis. Case was discussed in our institutional multidisciplinary tumour board and board’s decision was to go ahead with composite resection with neck dissection and reconstruction. After getting fitness from anesthesist, she underwent composite resection with right extended hemi mandibulectomy with right Modified radical neck dissection (Type III) with reconstruction by pectoralis major my cutaneous flap with tracheostomy. Microvascular free fibula flap was advised to the patient and her relatives, however, they opted for pedicled flap. Her postoperative course was uneventful and she was discharged on 7th postoperative day. Tracheostomy was decannulated on 12th postoperative day. Final histopathology report was suggestive of 8th edition AJCC staging as pT2 pN3b pM0 (Tumour size (Both) was < 2cm>
Synchronus SCC are aslo described as second primary tumours. They grow at the same time with primary SCC or within 6-month period of primary SCC. Warren and Gates and Moertel described the criteria of synchronous tumour as follows (1) all the tumours had to be histologically malignant (2) all had to be distinct masses separated by normal tissue at least by 2 cm (if the intervening mucosa demonstrates dysplasia, it is considered as multicentric primary) (3) the possibility that the tumours could be metastatic had to be excluded histologically. Slaughter et al. [ 4] had proposed the theory of “field cancerization” whereby multiple tumours could originate independently in an area of epithelium pre‑conditioned to cancer development by long‑term exposure to carcinogens. The alternate theory is that multiple tumours in the head and neck are of common clonal origin, and has gained support as a result of the detection of identical genetic alteration in these tumours [ 9].
A study by Dissanayaka WL et al [ 6], reported 100% male predominance of synchronous SCCs, with no synchronous occurrence in female patients. Contradictory to it, our index case is a female. The most common site of occurrence of synchronous SCCs is tongue (33.3%) followed by buccal mucosa (26.7%) [ 3]. Our index case had lesions involving right lower alveolus which is considered to be a rare site [ 7]. The reported age for synchronous SCC is more than 40 years which matches with our index case’s age i.e., 58 years. Tobacco and alcohol are considered as the most carcinogenic agents involved in field cancerization of the epithelium which leads to pronounced genetic changes, ultimately resulting in synchronous and metachronous cancers. Synchronous SCCs are more likely to occur if the index tumour is located in the lower part of the oral cavity (floor of mouth, lower alveolus, retromolar triangle) than if the tumour is located in the upper part of the oral cavity (buccal mucosa, tongue or palate). Our Index case had primary tumour located in lower alveolus. As per the reported case series, onset of synchronous SCC decreases the 5-year survival by 18-30% as compared to those with only a single primary tumour [ 3].

Over the last decade, there is an increasing trend of cases of multiple primary oral SCC. These cases need special attention as synchronous or metachronous cancers decreases the overall survival rate. A complete clinical examination of the oral cavity, oropharynx and larynx is necessary to avoid missing of second cancer. As the disease is aggressive, the treatment plan should be aggressive. Most of the cases of synchronous cancer requires adjuvant treatment. A periodic follow up protocol should be planned for these patients as chances of recurrences are more. Our index case had completed adjuvant treatment and she is in periodic follow up with us. She had been explained the nature of synchronous SCC. Thus, this is a rare case of synchronous oral squamous cell carcinoma involving lower alveolus in a female patient.
When a metachronous SCC develops after the complete treatment of primary SCC, a multidisciplinary treatment approach is necessary to address the tumour with aggressiveness as this cancer will be more resistant and aggressive. Hence a long-term surveillance is mandatory to detect the local recurrence of the primary tumour and to monitor the therapy and its complications. Metachronous or synchronous SCC diagnosis is purely histopathological. Thus, biopsy of the second primary tumour is mandatory for final confirmation.
Synchronous squamous cell carcinomas of the oral cavity are considered an aggressive and resistant variety. They metastasize earlier as compared to primary and requires an aggressive treatment strategy. Lower alveolus synchronous cancer in females is an extremely rare scenario.