
Case Report | DOI: https://doi.org/10.58489/2994-2624/006
*Corresponding Author: Veena Asthana
Citation: Chirag Ahuja, Veena Asthana, Ranjit Kumar, (2023) Anaesthetic precautions in Hydatid Disease. International Journal of Anesthesiology and Practice. 2(1). DOI:10.58489/2994-2624/006
Copyright: © 2023 Veena Asthana, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 31 December 2022 | Accepted: 16 January 2023 | Published: 20 January 2023
Keywords: Echinococcus Granulosis, found in dogs (Definitive Host), Sheep,cattle,goats
Hydatid disease is a serious parasitic infestation by a larval stage of tapeworm Echinococcus Granulosis, found in dogs (Definitive Host), Sheep,cattle,goats[1]. It is also known as cystic echinococcosis.
When a person comes in direct contact with the feces (infected via the eggs from the tapeworm) of an infested dog or consumes food and milk contaminated by the same,may develop hydatid disease[1]. The cyst formed by the disease are,mainly found in liver (75%),lungs( 30% ). The spinal involvement is usually caused by directextension from pulmonaryor abdominal invasionsand rarely begin primarily in the vertebralbody.
In the endemic areas,hydatid disease is one of the expectedcauses of spinalcord compression and the diagnosismay remain obscure until symptomsappear due to root and cord compression [2,3]
Symptoms of hydatid disease are radiculopathy, myelopathy and local pain which can further result in destructive bony lesions, pathological fracture and consequential cord compression[4]. Preoperative evaluation is necessary because the rupture of the cyst may result in anaphylaxis and recurrence. It may also produce and produce cough,chest pain, hemoptysis or haemodynomic instability.
A 44-year-old man, presented with gradually increasing back pain and progressively increasing difficulty in walking since three months. Pain was insidious in onset, gradually progressive and was radiating towards bilateral lower limb. He also complained of numbness, altered sensations in both legs
General physical examination revealed decreased Air entry on left lower lobe. On Neurologicalexamination the power was reduced to Grade three in both the lower limbs and there was loss of sensations, especially to pain and fine touch. The superficial abdominal and cremastric reflexes were present and plantars were extensor bilaterally. The knee and the ankle jerk were exaggerated with bilateral ankle clonus.
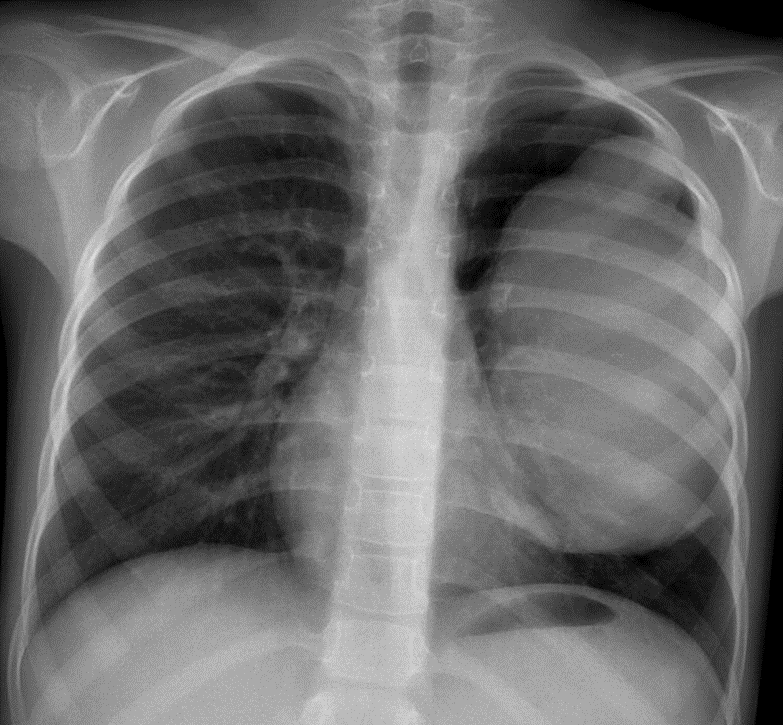
On MRI multifocal lobulated cystic lesion with peripheral and septal enhancement in thoracolumbar (D10-L1) and lumbosacaral canal (L5-S2) intradural location (? parasitic cyst)cystic multiseptate structures were also seen on right upper hemithorax, left hemipelvis, perimedullary cisternof brain. Chest x-rayalso revealed a large roundedopacity with smoothwall in left upper and middle zone, which was s/o Hydatid cyst
Patient went under T10-L1 + L5-S1 laminectomy procedure with total excision of cysts. They were multiple in numberand grey coloured,soft in consistency with ,highly Vascular,and densely adhered to cord and roots.
2 units of PRBC were arrangedand high-risk consent was taken Patientwas taken into OT, all monitors were attached Vitals- HR-86/min, BP-128/84mmHg, SpO2- 100% Two 18 G cannula was secured on both the forearms. Induction was with- Inj FENTANYL 100 mcg + Inj XYLOCARD 60 mg + Inj PROPOFOL 100 mg IPPV was done Inj VECURONIUM 7 MG IV was given.Laryngoscopy with blade #3 was done and flexometallic ETT was inserted#8.5/22/5 and securedin place.
Patient was then taken into a prone position; All the IV cannulas were secured properlyand all the bony prominences were padded adequately and procedure lastedfor 2 hours.
While removing the cysts due care was taken to prevent rupture of the cyst, epinephrine, atropineand sodium bicarbonate, dexamethasone, and salbutamol(inhaler) were kept handyto treat anaphylactic reaction if it presented intraoperatively. The other hand surrounding the surgicalfield, was packedwith mops to prevent local leak.
It was taken care of that Scolicidal solutions, such as hypertonic saline and hydrogenperoxide, were not used duringsurgery to preventchemical injury to cord.
After 1 hour of induction patient showed a sudden dip in blood pressure to 98/60mmHg which was immediately managed by giving Inj methylprednisolone 100mg IV Stat after which blood pressurewas recovered within15 min.
Postoperative period was uneventful and tab Albendazole was given for a periodof
three months. There was complete regain of sensation in two to three weeks, although motor functions graduallyover six weeks.
Patient was successfully extubatedand shifted to the recoveryroom. Postoperative period too remaineduneventful. Patient had significant pain relief and reduced spasticity.
Anaphylactic reaction is a systemic event that affects many organs and can be life-threatening. Anaphylaxis during anesthesia and the per-operative period is rare.
Anaphylaxis includesnausea, vomiting, urticaria, angioedema, bronchospasm, upper airway obstruction, cardiovascular collapse. The mortality rate due to anaphylaxis is between3%-6% [4]
During excisional surgery, an anaphylactic reaction may occurafter the rupturing of the cyst. The causeof the death in hydatidcyst rupture is due to anaphylaxis-related complications.The incidence of intraoperative anaphylaxis due to hydatid cyst has been reported as 0.2%-3.3%, and it has mediated by Ig E-mediated type 1 hypersensitivity reaction [4]. General anesthesia is covering almost all the clinical symptoms of anaphylaxis. Urticaria, hypotension,bronchospasm,bradycardia are the main symptoms that can be observed.
Massive fluid resuscitation with crystalloid or colloid, vasopresso drugs
(Adrenaline, noradrenaline), glucocorticoids, H1and H2 receptor blockers are used in the treatment of anaphylactic reaction. If anaphylaxis develops, all medications should be used and the operation should stop, and 100% oxygen treatment should start. The first-line treatment of perioperative anaphylaxis is epinephrine (vasopressor). Glucocorticoids are used to reduce the late effect of anaphylaxis. Some studies reportedthat preoperative H1 and H2 receptor blockersare useful in hydatid cyst surgery to prevent anaphylaxis [1]
In conclusion the management of a hydatedcyst needs a thorough understanding of the physiology and the proper positioning of the endobronchial tube and continuous monitoring of the saturation, ventilation, haemodynomics and the blood gases to prevent any associated complications.