Archive : Article / Volume 2, Issue 1
- Case Report | DOI:
- https://doi.org/10.58489/2836-2330/014
Isolated Acute Rheumatic Pancreatitis- A Case Report
Morning Star hospital, Marthandam, Kanyakumari District, India
Ramachandran Muthiah. Morning Star hospital, Marthandam, Kanyakumari District, India
Ramachandran Muthiah. Isolated Acute Rheumatic Pancreatitis- A Case Report. J. Clin. Med. Rev. Vol 2, Iss 1. (2023). DOI: 10.58489/2836- 2330/014
© 2023 Ramachandran Muthiah, this is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
- Received Date: 14-12-2022
- Accepted Date: 23-12-2022
- Published Date: 06-03-2023
Acute abdomen, Pancreatitis, ASO titer, Elevated pancreatic enzymes, Antibiotics
Abstract
To emphasize the role of antibiotics in acute pancreatitis as prophylactic and therapeutic benefits. A 32-year-old obese male was admitted with acute abdomen in the emergency room. He was supported with intravenous fluids and the blood chemistry revealed elevated amylase and lipase levels, raised ESR and a positive ASO titer test. CT abdomen suggested interstitial edematous pancreatitis (IEP) and no fluid collection. Patient was treated with IV cefotaxime and metronidaziole and his condition remarkably improved with therapy and blood parameters returned normal at the end of 4 weeks and follow up CT revealed no abnormal findings and symptom free thereafter. Acute pancreatitis is usually a sterile inflammatory process caused by chemical autodigestion of pancreas. The edematous form of acute pancreatitis needs to correct its etiological factor to avoid recurrence. It is observed as an initial manifestation of group A beta hemolytic streptococcal infection in this patient and antibiotics play a role as curative and prophylactic in selected cases.
Introduction
Acute pancreatitis is a condition where the pancreas becomes inflammed (swollen) over a short period of time. Most people with acute pancreatitis start to feel better within about a week and have no further problems. It is sometimes associated with a systemic inflammatory response that can impair the functions of other organs, can go on to develop serious complications. Thus, there is a wide spectrum of disease from mild (80%), where patients recover within a few days, to severe (20%) with prolonged hospital stay, the need for critical care support, and 15-20% risk of death if patients have organ failure during the first few weeks of illness [1].
It occurs with an estimated incidence of 10-40 per 100,000 per year in the UK [2]. An increase in the annual incidence for acute pancreatitis has been observed worldwide varies between 4.9 and 73.4 cases per 100,000 [3,4]. Every year, there are 275,000 hospitalisations for acute pancreatitis in the United States. In 2009, it is the most common gastroenterology discharge diagnosis with a cost of 2.6 billion dollars.
The evolving issues of antibiotics, nutrition, endoscopic, radiologic, surgical and other minimally invasive interventions will be addressed on early management to decrease morbidity and mortality.
Some studies have suggested that the administration of prophylactic antibiotics reduces the risk of pancreatic necrosis becoming infected [5]. Abdominal pain is the presenting manifestation of acute rheumatic fever [6], usually precedes the other rheumatic signs and it is the consequence of rheumatic inflammatory process affecting the pancreas in this patient and so this case had been reported.
Case Report
A 32 years old male was admitted with sudden onset of severe abdominal pain and he was found to be toxic and emaciated. His pulse rate was 114 bpm, blood pressure 90/60 mmHg and temperature 100.4∙F. Physical examination revealed distended abdomen with tenderness in the epigastric region. He had a history of alcoholic drinks occasionally. He was on anticonvulsants (phenytoin sodium 100mg twice daily) for the past 4 years as he suffered 2 to 3 episodes of seizure attacks before and his CT brain revealed normal earlier. On admission, his serum amylase was 548 IU/L (normal 10 to 96 IU/L). The total leukocyte counts 7190 cells/cumm blood (normal 4000 to 10000/cumm of blood), neutrophils 65.8% (normal 40 to 75%), lymphocytes 26.3% (normal 25 to 35%), monocytes 4% (normal 3.5 to 11.5%), eosinophils 3.5% (normal 2 to 6%), basophils 0.4% (normal 0 to 1%). ESR (Erythrocyte sedimentation rate) 26 mm in one hour (normal 0 to 14 mm per hour). Serum bilirubin (total) 1.2mg/dl (normal 0.4 to 1.2mg/dl). Random blood glucose 98mg/dl (normal 60 to 125 mg/dl). Total cholesterol 180mg/dl (normal 150 to 220 mg/dl), serum triglycerides 270mg/dl (normal 50 to 150 mg/dl). Serum SGOT (AST) 88 IU/L (normal 5 to 41 IU/L, SGPT (ALT) 78 IU/L (normal 5 to 50 IU/L). The renal parameters and serum electrolytes were within normal range. Serum lipase was highly raised as 1476 IU/L (normal < 60>Figures 1 and 2, with normal pancreatic parenchyma and no significant ductal dilatation and calcification. The liver and gallbladder appear normal, no evidence of gallstones and no fluid collections. The abdominal distension subsided on 4th day and the patient was advised to resume semisolid liquid diet, tendor coconut water, fruits and smashed vegetables without chillies slowly. The milk products were avoided. His condition began to improve thereafter. After one week of treatment, the amylase level decreased to 303.1 IU/L and lipase level becoming 240.4 IU/L, AST 84 IU/L, ALT 80 IU/L. Then one week thereafter, the amylase level reduced to 151.2 IU/L, lipase level 128.4 IU/L, AST 49 IU/L and ALT remaining high as 89 IU/L. At 3rd week, AST 36 IU/L, ALT 51 IU/L, amylase 148 IU/L, lipase 115 IU/L and ASO titer 288.5 IU/ml.
The treatment continued and at the end of 4 weeks, the amylase 69 IU/L, lipase 31 IU/L and ASO titer became negative. The CT abdomen revealed no fat stranding and the pancreas appeared normal. The patient get discharged to home and advised to avoid alcohol and fatty foods thereafter. The patient was symptom free and healthy on one year follow up, advised lifelong penicillin prophylaxis with oral penicillin V 250mg twice daily to prevent recurrent attacks of pancreatitis. Since he is obese with body mass index (BMI 32%), regular exercise programmes and diet control were advised for weight reduction with periodic medical check-up.
The RT PCR for COVID 19 infection (reverse transcriptase polymerase chain reaction test) was negative at present and it was not done initially since unknown at the time of presentation.

Figure 1: showing the mild increase in densities of ‘fat stranding’ as ‘mistiness’ or ‘hazy streaky densities’ representing the inflammatory changes in the peripancreatic fat near the uncinate process of pancreas. extending towards tail region and perinephric area suggesting “acute interstitial edematous pancreatitis (IEP)”
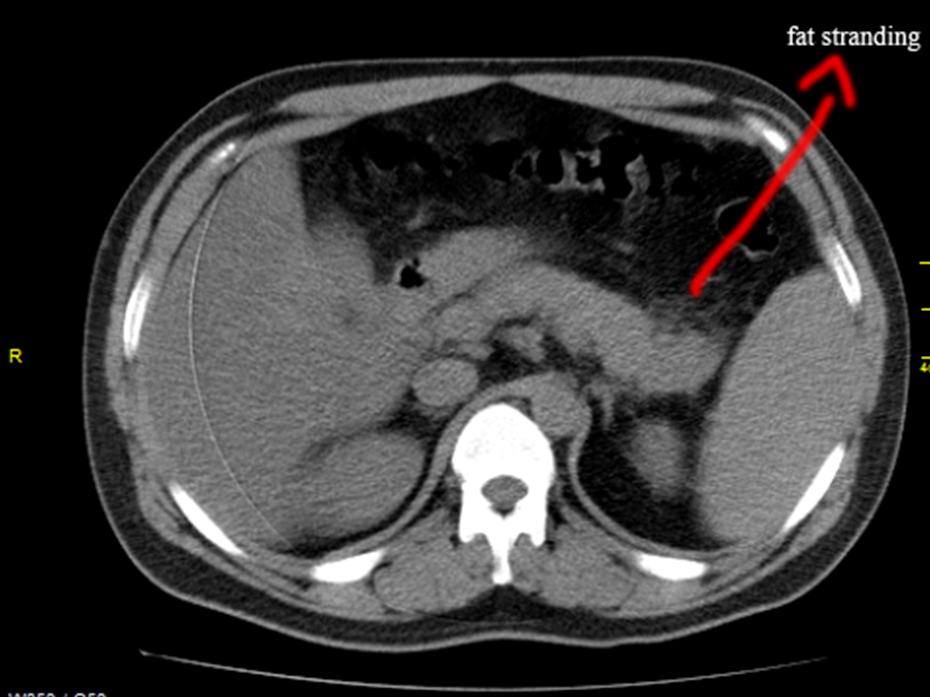
Figure 2: showing the ‘mistiness’ (fat stranding) in the tail region of the pancreas
Discussion
Etiopathogenesis
The pancreas is a secretory organ with both endocrine and exocrine functions and the main functional unit is the acinar cell, which comprises the parenchyma of the gland. Exocrine products from the acinar cells are secreted into a tubular system and the digestive enzymes are released via the pancreatic duct into the small intestine where they are activated to break down the fats and proteins. The digestive hormones (insulin & glucagon) produced by the pancreas are released into the blood stream where they help to regulate the blood glucose level.
Normally, digestive enzymes released by the pancreas are not activated to break down fats and proteins until they reach the small intestine. Trypsin is a digestive enzyme produced in the pancreas in an inactive form and ethanol molecules affect the pancreatic cells, triggering them to activate trypsin prematurely. When the digestive enzymes are activated in the pancreas, inflammation and local damage as ‘acinar cell destruction’ histologically occurs, leading to pancreatitis. Neutrophil polymorphs and macrophages infiltrate the pancreas and release their own proteases, free radicals, and cytokines which compound the vicious cycle of tissue damage and inflammation, inducing an ‘acute systemic inflammatory response syndrome (SIRS)’ and organ damage. The patient may become dehydrated and then heart, lungs, kidney fail. In very severe cases, pancreatitis can result in bleeding into the gland, leading to shock, serious tissue damage, infection, fluid collections and sometimes death.
There are many causes of pancreatitis as obstruction of the secretory tree or direct parenchymal cell damage. The gallstones, infection and alcoholism are the most common causes of acute pancreatitis. In recurrent acute pancreatitis, Oddi sphincter manometry is performed and a basal sphincteric pressure > 40 mmHg [7] is the most common abnormal finding described in 30-40% of cases. DIP (drug induced pancreatitis), which is an overlooked diagnosis in the clinical setting, must be rigorously considered whenever patients are on a set of new drugs and presenting with even, minimal symptoms and signs of acute pancreatitis.
Drugs are responsible for 0.1% - 2% of acute pancreatitis incidents. The majority of drug-induced pancreatitis cases are mild to moderate in severity; however, severe and even fatal cases can occur. The newly emerged drugs like propofol infusion, antidiabetics (GLP1- Glucagon-like Peptide-1 Receptor) agonists and DDP4 (Dipeptidyl Peptase IV) inhibitors and SGLT2 (Sodium-glucose Cotransporter-2) inhibitors, particularly, canagliflozin), antibiotics (minocycline), antihypertensive agents (enalapril, lisinopril, captopril, ramipril, perindopril, and less frequently angiotensin receptor blockers), proton pump inhibitors (omeprazole, pantoprazole, and lansoprazole), anticancer drugs (nivolumab, pembrolizumab, ipilimumab), the newer TKIs (Tyrosine kinase inhibitors- vemurafenib and ponatinib), proteasome inhibitors (bortezomib), and non-selective TACE (Trans arterial chemoembolization), and direct-acting antiviral therapies (DAAs) of hepatitis C virus along with ribavirin and currently, more than 500 drugs have been reported in the World Health Organization database as offenders of acute pancreatitis. The onset of drug-induced pancreatitis after initiation of medications ranges from a few months to several years, with a median of 5 weeks; onset after rechallenge can occur within hours. The latency between initiation of the offending drug and developing acute pancreatitis can be short (less than 24 h), intermediate (1-30 days), and long (more than 30 days). According to Badalov classification system of drug induced pancreatitis, the latency is described as consistent with the drug-related pancreatitis when 75% of cases were related to any of the previously mentioned groups. Potential mechanisms for drug-induced acute pancreatitis include pancreatic duct constriction, immune-mediated inflammatory response, direct cellular toxicity, arteriolar thrombosis, metabolic effects, hypersensitivity (Idiosyncratic) reactions, localized angioedema effect in the pancreas and Influence of medication on the bile flow.
The onset of acute pancreatitis induced by statins has been observed from hours to years after treatment. Because of the variance in the latency period, the mechanism may be related to a direct toxic effect to the pancreas and the accumulation of a toxic metabolite. Other mechanisms of action of statin-induced acute pancreatitis are speculated to be associated with rhabdomyolysis, myalgia, and/or metabolism or drug interactions through cytochrome P-450 3A4 (CYP3A4) In several case reports, either myalgia or rhabdomyolysis occurred before development of acute pancreatitis and pravastatin does not metabolize CYP3A4, it may have fewer case reports of drug-induced acute pancreatitis than other statins. A possible mechanism of action for angiotensin converting enzyme (ACE) inhibitor–induced acute pancreatitis is proposed to follow the mechanism of local angioedema of the pancreatic duct as they decrease the degradation of bradykinin which causes increased vascular permeability in the pancreas and can result in pancreatic edema. In addition, angiotensin II receptors may be important in regulating secretion and microcirculation within the pancreas.
The onset of acute pancreatitis is sudden. The patient presents with epigastric abdominal pain, vomiting and collapse. The pain is steady, boring and severe and often made worse by walking and lying supine and better by sitting and leaning forward. Patients are restless and bringing their knees to their chest in an effort to alleviate the pain. The pain usually radiates to back, but may radiate to the right or left. Marked epigastric or diffuse tenderness on palpation with rebound tenderness and guarding is present in severe cases. The abdomen is often distended and tympanic, with bowel sounds decreased or absent in severe disease. The vital signs may be normal, but hypotension, tachypnea, tachycardia and low grade fever are often observed, especially with widespread pancreatic inflammation and necrosis. Jaundice is a common finding. In 3% of patients with severe acute pancreatitis, flank ecchymosis (Grey Turner sign) or periumbilical ecchymosis (Cullen sign) develops and is suggestive of retroperitoneal hemorrhage. Some patients display alterations in mental status, more common in drug-induced acute pancreatitis and reflects exposure to drugs or to ethanol but may also result from hypotension, hypoxemia, or the massive release of toxic agents from the inflamed pancreas. The condition has to be differentiated from other diseases producing acute abdomen such as acute appendicitis, perforated peptic ulcer, acute cholecystitis and infarction of intestine following sudden occlusion of the mesenteric vessels.
Acute pancreatitis is associated with multiple infections as shown in Table 1. In most reports, bacteria are considered important only in late stage of pancreatitis and not as a primary etiological agent. Pancreatic ischemia is rare due to its rich perfusion from superior and inferior pancreaticoduodenal arteries and ischemia may results from vasculitis due to rheumatic inflammation and alcohol induced ‘microcirculatory impairment’ potentiated by smoking.
When pancreatic ischemia occurs, its tissues begin to die as necrosis and when it happens, the pancreas can become infected and it’s spread into the blood causes ‘sepsis syndrome’ mimicking SIRS in its early course of acute severe pancreatitis. The risk of infection is associated with degree of pancreatic necrosis. Patients with < 30> 50% have 46.5% of risk of infection [8]. Infection of necrotic tissue by bacteria carries high morbidity and mortality [9].
Infections Can Result from a Variety of Sources
- Bacterial translocation- from small bowel and colon through transmural colonic migration is a major source of infection in necrotizing pancreatitis [10]. Endotoxemia resulting from the release of components of gram-negative bacteria from the gut is common in patients with acute pancreatitis. The bacterial translocation from the gut lumen to mesenteric lymph nodes and subsequent hematogenous dissemination could be a possible mechanism of the development of pancreatitis. Impaired body defences predispose to translocation of gastrointestinal organisms and toxins with subsequent secondary bacterial infection.
- Hematogenous spread
- Biliary sources- bile duct stone or gall bladder infection ascending from duodenum via the main pancreatic duct can lead to infected pancreatic necrosis.
Most pathogens in pancreatic necrosis are gastrointestinal gram-negative bacteria (Escherichia coli, Proteus, Klebsiella pneumonia), occur via disruption of intestinal flora and damage to bowel mucosa. However, gram positive bacteria (Staphylococcus aureus, Streptococcus faecalis, enterococcus), anaerobes, occasionally fungi have also been found and 25% are polymicrobial infection [11].
Streptococcus pyogenes (Lancifield group A β hemolytic streptococci, a gram positive, non-motile, non-spore forming coccus is the causative organism of Rheumatic fever which is a systemic disease affecting the periarteriolar connective tissue. Acute pancreatitis is an abrupt inflammation of the pancreas and a potential pathway of inflammatory response induced by the cytokines TNF-α and IL-6 (Interleukin 6) is responsible for the development of inflammation. During bacterial invasion, the M1 protein (Matrix protein) is shed from the surface of streptococcus pyogenes into the blood stream causing widespread activation of host innate immune cells. The ‘superantigens’ (streptococcal pyrogenic exotoxin (Spe) mediate a non-antigen specific binding between T cell receptors and major histocompatibility complex class II molecule on antigen presenting cells. Consequently, the monoclonal cells are activated to produce large amounts of cytokines, and expression of TNF-α (tumor necrosis factor alpha) in the pancreatic islets may induce an inflammatory response in the pancreas and also cause dilatation and altered permeability of blood vessels, leading to acute lung damage, hypoalbuminemia, ascites and shock in susceptible individuals [12].
Among immunocompetent individuals, mumps and coxsackie B virus are the most common cause of pancreatitis. Recently, gastrointestinal manifestations of COVID 19 (corona virus disease 2019), caused by SARS-Cov-2 (severe acute respiratory syndrome corona virus 2), a family of single-stranded RNA virus are increasingly being recognized and its pathogenesis is thought to be mediated by angiotensin converting enzyme (ACE2) receptor on the host cells, which are highly expressed in pancreatic islets [13]. Acute pancreatitis can occur due to direct cytopathic effects of local SARS-Cov-2 replication or indirectly by immune mediated inflammatory response induced by the virus [14]. It has been reported that there is 17% incidence of pancreatic damage occurred in COVID 19 patients [15,16] and CT revealed the changes of interstitial edematous pancreatitis in majority of cases rather than necrotizing pancreatitis [17].
|
Mumps |
|
E. coli |
|
Coxsackie B virus |
|
Candida |
|
Hepatitis B |
|
HIV |
|
Varicella-zoster virus |
|
Leptospirosis |
|
Cytomegalo virus (CMV) |
|
Covid 19 virus |
|
Legionella (L. pneomophila found in plumbing, Shower heads, water storage tanks) |
|
Shigella |
|
Salmonella |
|
Parasites |
|
Toxoplasma |
|
Ascariasis |
|
Clonorchis sinensis |
Table1: Infectious agents causing pancreatitis
n 1992, the Atlanta classification for acute pancreatitis was introduced to classify its various manifestations [18]. The Atlanta classification divides acute pancreatitis into two groups: interstitial edematous acute pancreatitis and necrotizing acute pancreatitis. The first category is characterized by pancreatic parenchymal and peripancreatic inflammation without necrosis, while the latter category involves inflammation and some degree of necrosis. Relatively little necrosis or organ failure is seen in mild acute pancreatitis, but severe acute pancreatitis is characterized by extensive necrosis complicated by intrapancreatic thrombosis and vascular disruption. The revised classification described two distinct phases of acute pancreatitis, a first or early phase that occurs within the first week of onset of disease and a second or late phase that takes place after the first week of onset [19] and introduced a new terminology of fluid collections as acute peripancreatic fluid collection (APFC) and acute necrotic collections (ANC).
During the first week of acute pancreatitis, the pathologic condition in and around the pancreas progress from early inflammation with variable degrees of peripancreatic edema and ischemia to resolution or to necrosis of pancreas or surrounding fatty tissue. Over the course of first week, organ failure either resolves or become more severe. The organ failure that resolves in 48 hours are considered to have mild pancreatitis without complications [20]. Severe acute pancreatitis in the first phase is defined as organ failure that lasts more than 48 hours or death. Expansion of systemic inflammatory response syndrome and ensuing multiorgan failure is responsible for many deaths during this phase. The late phase begins after the first week, may extend for weeks to months and is characterized by increasing necrosis, infection, and persistent multiorgan failure [21]. Local complications may manifest systemically with bacteremia and sepsis when necrotic tissue becomes infected.
Laboratory Parameters
The pancreas produces elevated levels of enzymes, the amylase, lipase and trypsinogen, all derived from pancreatic acinar cells during acute pancreatitis. Serum pancreatic enzyme measurement is the ‘gold standard’ for the diagnosis of acute pancreatitis (AP) [22]. Serum amylase usually rises within 6 to 24 hours, peaks at 48 hours, and return to normal within 3 to 7 days [23] and lipase rises within 4-8 hours, peaks at 24 hours and decreases to normal in 8 to 14 days [24]. In this patient, both serum amylase and lipase persistently elevated up to 4 weeks with an early peak at 24 hours of onset of symptoms. The biochemical criteria are usually sensitive for detecting acute pancreatitis (55 to 100%) and its specificity is very high (93 to 99%). Amylase or lipase levels more than three times of the upper limits of normal (300 IU / litre-1 for amylase and 600 IU litre-1 for lipase are diagnostic of acute pancreatitis and serum lipase has been recommended as assay of choice [25] since its concentrations are increased for up to 14 days after the onset of pancreatitis, and appears to be more sensitive and specific than amylase.
Trypsinogen is the zymogen of the pancreatic enzyme trypsin and in acute pancreatitis, its concentration in serum and urine rises to high levels within a few hours and decrease in 3 days. Urinary trypsinogen 2 dipstick test is a rapid and noninvasive bedside test with a reasonable sensitivity 82% and specificity 94% for acute pancreatitis [26] if positive (> 50 ng/ml).
Many clinicians consider the C reactive protein (CRP) as the gold standard for disease severity assessment [27], but its peak levels are reached only after 48 to 72 hours. The CRP at 24 hours ≥ 21 mg/dl (≥ 210 mg/l) indicates severe disease and its level on 3rd day ≥ 150 mg/l can be used as a prognostic factor for severe acute pancreatitis. Resistin is a newly identified peptide hormone, secreted by adipocytes that can cause obesity and hypertriglyceridemia, due to its association with insulin resistance. It is an important cytokine in inflammatory reactions, in the regulation of other cytokines [28] and it is better to predict severe acute pancreatitis on day 3 and for the development of pancreatic necrosis than CRP or WBC levels. It has similar accuracy with Acute Physiology and chronic health evaluation II (APACHE II) score in predicting persistent organ failure (POF) and leptin has a weak correlation with POF [29].
PCT (procalcitonin) may be valuable in predicting the risk of developing infected pancreatic necrosis. It is an inactive 116 amino acid propeptide of the biologically active hormone calcitonin, which was first described to have significantly increased concentrations in bacterial and fungal infections [30]. Procalcitonin is the most sensitive laboratory test for detection of pancreatic infections and low serum values appear to be strong negative predictor of infected necrosis. A procalcitonin value of 3.8 ng/ml or higher within 96 hours after the onset of symptoms indicated an infected pancreatic necrosis with sensitivity of 93% and a specificity 79% [31].
A laboratory “acute pancreatic screen” to determine the etiology also include the detection of viral antibodies, especially for corona virus. Streptococcus pyogenes produces various exotoxins such as streptolysin O that can act as antigens and the affected individuals produce specific antibodies against streptolysin O (antistreptolysin O (ASO)). Determination of these antibodies is very useful for the diagnosis of streptococcal infection and their relative effects. An elevated ASO titer > 200 IU/ml may indicate an acute streptococcal infection and, in this patient, the ASO titer was raised up to 440 IU/ml at the time of admission.
Advanced laboratory analysis for patients < 40 years of age includes the detection of α-1-antitrypsin phenotype, CFTR (cystic fibrosis transmembrane conductance regulator) gene analysis, a sweat chloride test, trypsin gene studies, and duodenal aspiration for microcrystals, The best indicator of bile duct stones is a serum total bilirubin > 1.35 mg/dl on the second day of admission [32]. The level of tumor marker, CA (cancer antigen) 19-9, should be measured in patients > 40 years of age. An elevation on serum Immunoglobulin G subclass 4 level (IgG4 > 135 mg/dl) is typical of autoimmune pancreatitis (AIP), however, mild ( < 2 fold) elevations are seen up to 10% of subjects without AIP including pancreatic cancer.
Predictors of Severity
It is unable to predict which patients with acute pancreatitis will develop severe disease and different scoring systems showed similar predictive accuracy for the severity of acute pancreatitis, but the APACHE-II score demonstrated the highest accuracy [33].
It was able to identify patients at increased risk of mortality prior to the onset of organ failure [34]. The BISAP score of 2 was a statistically significant cutoff value for the diagnosis of severe acute pancreatitis, organ failure, and mortality as shown in Table 2.
|
Blood urea nitrogen level > 25mg/dl (89 mmol/l) |
|
Impaired mental status (Glasgow coma score < 15) |
|
Systemic inflammatory response syndrome |
|
Age > 60 years |
|
Pleural effusion |
Table 2: Showing the Bedside index of severity of acute pancreatitis (BISAP) [35].
(A score of 3 points is associated with 5.3% rate of hospital death, 4 points with 12.7%, and 5 points with 22.5% of deaths)
The systemic inflammatory response syndrome (SIRS), originally adopted to predict the development of organ failure with sepsis, currently the most important predictor of prognosis [36] and it requires at least two of the following criteria as shown in Table 3. It identifies the risk very early in the course of disease and can be assessed quickly in the emergency department.
|
Heart rate |
> 90 bpm |
|
Core temperature |
< 36◦C or > 38◦C |
|
White blood cells |
< 4000 or >12000/mm3 |
|
Respirations |
>20/mm |
Table 3: Showing the criteria of SIRS (systemic inflammatory response syndrome) [36]
The emerging biomarkers to distinguish septic and non-septic etiology of SIRS include TREM 1 (Triggering receptor expression on myeloid cells 1), DcR3 (‘Decoy receptor 3’ belongs to tumor necrosis factor family) and suPAR (Soluble urokinase type plasminogen activator receptor) [37].
CT (Computed Tomography) Imaging
The peripancreatic inflammatory changes are the most common CT findings in 88% of cases of acute pancreatitis, seen in mysentry, greater omentum and transverse mesocolon as shown in Figures 1 & 2 and the second most common finding is ‘pancreatic contour irregularity’, seen in 80% of cases. Pancreatic parenchymal necrosis alone is seen in < 5>
The pancreatic parenchyma and peripancreatic fat begin to liquefy slowly and the extent of necrosis is divided with 3 categories as >30%, 30 to 50%, >50% of gland involved [39]. The modified CT grading system described only two categories as < 30>30% [40]. Areas of no or poor attenuation indicates edema rather than necrosis and estimate to be < 30>
Ultrasound Imaging (USG)
It can be used to look for gallstones and abnormalities of biliary system and it does not emit radiation. It may difficult to visualize pancreas in presence of clear and free peritoneal fluid. A combination of endoscopy and high frequency ultrasound (EUS) may be useful if CT fails to detect the CBD (common bile duct) stones and it is highly sensitive for the diagnosis of PD (pancreatic divisum) than CT [42,43]. It is highly specific to diagnose pancreatic cancer and able to identify pancreatic masses as small as 2 to 3 cm [44].
MR (Magnetic Resonance) Imaging
It is helpful to visualize the distal common bile duct stones and also useful in patients with renal insufficiency to avoid contrast enhanced CT [45]. MR imaging or ultrasound may be used to determine the presence of nonliquefied material.
ERCP (Endoscopic Retrograde Cholangiopancreatography)
The endoscope, a thin flexible tube with a camera at the end can help to determine the exact location of gallstone. ERCP is recommended in the setting of acute pancreatitis with cholangitis, presence of jaundice and common bile duct obstruction. Autoimmune pancreatitis can be difficult to distinguish from pancreatic cancer on CT, but typically features ‘diffuse irregular narrowing of the main pancreatic duct’ on ERCP. The diagnosis of choledochocele is usually confirmed by ERCP. Endoscopically, the papilla has a “bulging” appearance and feels soft (pillow sign) when pressure is applied with the catheter tip [46]. Routine ERCP is advised for all patients with acute gallstone pancreatitis. ERCP should be considered in presence of persistently abnormal liver function tests (serum ALT > 150 IU/litre-1) and it cannot be recommended without cholangitis or common bile duct obstruction due to procedure related complications including acute pancreatitis, hemorrhage, perforation, sepsis, stricture, bile leakage with mortality in 6% of cases. It does not allow the evaluation of pancreatic parenchyma and less sensitive to detect masses, chronic pancreatitis and microlithiasis [47]. Because of these reasons, ERCP is not advised in this patient.
MRCP (Magnetic Resonance Cholangiopancreatography)
It gives detailed information about the hepatobiliary and pancreatic systems [48], recommended for patients with recurrent acute pancreatitis of unknown cause to assess for pancreatic divism, choledochocele, anomalous pancreatobiliary junction or annular pancreas.
Secretin Stimulated MRCP (sMRCP)
Secretin is injected intravenously, causing the main pancreatic duct to secrete fluid, which improves the visualization of pancreatic ducts [49] and should be preferred for diagnosing pancreatic divism.
Therapeutic Aspects
The treatment planning is based on severity of pancreatitis. IEP (interstitial edematous pancreatitis) is usually self-limited and supportive measures alone suffice. Mild acute pancreatitis is moderately or severely painful. The first line treatment includes bowel rest, IV fluids to prevent dehydration and pain medications.
Pain Relieving Agents
All patients with acute pancreatitis must receive some form of analgesics in the first 24hrs and dilaudid (hydromorphone hydrochloride) is preferred over morphine or fentanyl in the non-intubated patient. Epidural analgesia may be considered in severe and acute critical care patients who require high doses of opioids for an extended period. Excessive sedation may worsen gut dysfunction with subsequent increase in intraabdominal pressure and intractable pain may necessitates EUS-guided celiac plexes block.
NSAIDs (non-steroidal antiinflammatory drugs) are the most promising group to attenuate the inflammatory response in acute pancreatitis. Rectal suppositories of 100 mg diclofenac or 100 mg indomethacin can reduce the incidence of post ERCP pancreatitis.
Chronic use of opioids causes spasm and dryness of pancreatic ducts, which in turn increases the inflammation and producing more pain. The “nonvalidated” medical therapies such as smooth muscle relaxers (calcium channel blockers or nitrates) may abort an attack if taken at the onset of symptoms. Oral pancreatic enzyme supplements which inhibit pancreatic enzyme secretion may be beneficial for pain control, especially in idiopathic chronic pancreatitis.
Bowel Rest
Bowel rest is needed for a few days, so that not to take any food or drinks by mouth until their condition improves, resolution of pain, awaiting normalization of pancreatic enzymes and even imaging evidence of resolution of inflammation before resuming oral feeding [50]. Several studies have shown that early oral feeding decreases the morbidity, mortality and infectious complications and it may begin as low- residue, low fat, soft diet when the patient appears to be improving as no tummy (abdominal) pain and found to be safe in mild acute pancreatitis [51].
Intravenous Hydration
The microangiopathic effects and edema of inflammed pancreas worsens the pancreatic hypoperfusion and decreases the blood flow, causes increased release of pancreatic enzymes, activating numerous cascades, leading to increased parenchymal necrosis and cell death [52]. Necrotizing pancreatitis is an ischemic event and the goal of volume resuscitation is to maintain pancreatic and intestinal microcirculation to prevent intestinal ischemia and subsequent bacterial translocation [53], to prevent severe complications such as pancreatic necrosis [54] and to minimize SIRS (systemic inflammatory response syndrome) to reduce the rate of organ failure, morbidity and death. So, early intravenous hydration during the first 12 to 24 hours with close monitoring is of paramount importance.
Hydration with isotonic crystalloid solutions are advisable and the lactated Ringer’s solution (20ml/kg bolus, followed by 3 ml/kg/hour improve outcome within 36 hours) appears to be more beneficial with antiinflammatory effect, resulting less SIRS compared to normal (0.9%) saline [55] and a better electrolyte balance, improved outcomes and more pH balanced since low pH activates the trypsinogen, makes the acinar cells more susceptible to injury. The use of normal saline in large volumes may lead to non-anion gap, hyperchloremic metabolic acidosis.
Continuous use of aggressive hydration over 48 hours seems to be associated with increased morbidity and mortality [56,57] and caution to avoid excessive resuscitation ( > 4 liters in 24 hours) due to complications such as volume overload, pulmonary edema (due to increased systemic permeability) and abdominal compartment syndrome [58]. Movement of fluid into the intracellular space (“third spacing”) occurs in acute pancreatitis and fluid resuscitation exacerbates it. The intraabdominal hypertension (sustained intraabdominal pressure > 12 mmHg) is associated with poor outcome. It should be monitored with transvescicular bladder measurements in those patients on mechanical ventilation and managed with ultrafiltration.
Enteral Feeding
Enteral nutrition is recommended to prevent gut failure and infectious complications. It is better to avoid solid foods for few days or longer since trying to digest solid foods could put too much strain on pancreas. When the solid foods need to be avoided, it may be given a special liquid food mixture through a tube as ‘enteral feeding’. The enteral feeding is cheaper, safer, and associated with fewer infective complications and a better overall outcome [59] with a decrease in organ failure and mortality [60].
Enteral feeding maintains the gut mucosal barrier and prevents its disruption and translocation of bacteria that seed pancreatic necrosis. Jejunal feeding is advocated if gastric feeding fails [61] as a result of duodenal ileus or obstruction from inflammatory masses and there is some evidence of superiority of ‘distal jejunal feeding’ in acute pancreatitis.
Total parenteral nutrition (TPN) should be considered only for patients who do not tolerate enteral feeding because of severe ileus since it is associated with infection and line-related complications.
Antibiotics
Prophylaxis refers to the administration of antibiotics in patients when no clinical infection is present with the intent to prevent pancreatic infection. Earlier trials suggested that prophylactic antibiotics might prevent infective complications in sterile necrosis [62], but subsequent trials failed to confirm this advantage and recent trials showed no decrease in mortality [63] and thus routine prophylactic antibiotics in acute pancreatitis may increase the incidence of infection with resistant bacteria or fungi and is no longer recommended [64].
CT rarely demonstrates gas in pancreas, lesser sac or retroperitoneum and it is only present in limited number of patients [65]. CT guided FNA (fine needle aspiration) for gram stain and cultures can guide to choose appropriate antibiotic regimen [66], but many centers abandoned the routine use of FNA because of high rate of false negative results. A more rational approach is to consider antibiotics if there is evidence of systemic sepsis or organ failure while recognizing the many signs of SIRS, especially with marked leukocytosis.
Since most infections in severe acute pancreatitis are caused by gram negative organisms, translocated from the gut, the carbapenems (imipenem and meropenem) have a good broad-spectrum coverage, excellent pancreatic penetrance [67] and it should be used only in critically ill patients due to the spread of carbapenem resistant Klebsiella pneumonia. Aminoglycosides are poor penetrance to pancreas and are of little use [68].
Acylureidopenicillins (azlocillin, mezlocillin, piperacillin, and furazlocillin) have an intermediate penetrance into the pancreas and are effective against gram negative organisms [69]. Among these antibiotics, only Piperacillin/tazobactam is effective against gram positive bacteria and anaerobes. Quinolones (ciprofloxacin and moxifloxacin) have good tissue penetration into pancreas with an excellent anaerobic coverage [70], but discouraged due to high rate of resistance worldwide. Metronidazole with its bactericidal spectrum focused almost exclusively against anaerobes, also shown good penetration into pancreas.
Fungal infection is a serious complication of acute pancreatitis and is associated with an increase in morbidity and mortality. When there is no clinical response to antibiotics, fungal infection can be suspected. Candida albicans is most frequent, followed by candida tropicalis and candida krusei. Fluconazole must be given if fungal isolates are identified.
Specific medical therapy
Insulin infusion (0.1 units/kg/hour in 24 hours until triglyceride level became < 500 mg/dl by keeping blood glucose level in normal range with dextrose solution) is effective in decreasing triglyceride by increasing the lipoprotein lipase (LPL) activity which can degrades chylomicrons and thus reduces serum triglycerides in acute pancreatitis. Insulin will also rest pancreatic tissue and may improves immunoparalysis via upregulating the expression of human leukocyte antigen on monocytes and decreasing cell apoptosis [71].
In certain cases, a successful method of treatment relies on apheresis for lowering of triglyceride levels. Plasmapheresis (PEX) improves the outcome not only by lowering triglyceride but also by removing proinflammatory markers and cytokines to downregulate the inflammatory process [72].
CBPT (combined blood purification therapy) is a two-step approach for the management of acute severe pancreatitis involving plasmapheresis and continuous venovenous hemofiltration (CVVH) and shown to improve mortality and lowering of inflammatory markers in severe acute pancreatitis irrespective of its etiology [73].
HVHF (high volume hemofiltration) and hemoperfusion (HP) is considered when plasmapheresis is not available and it removes the proinflammatory cytokines in addition to lowering triglyceride level.
Purified apoC-II infusion has yielded transient normalization of triglyceride levels and clinical improvement in pancreatitis patients with apoC-II deficiency. Medium-chain triglycerides have also been used to prevent acute hyperlipidemic pancreatitis during pregnancy as their absorption doesn’t require chylomicron formation. Anti-oxidant therapy (selenium, beta-carotene, vitamin C and α-tocopherol) has been used with success in the reduction of recurrent pancreatitis episodes in patients with familial lipoprotein lipase deficiency who remained markedly hypertriglyceridemic after medical therapy. It is postulated that the antioxidants might protect the pancreatic acinar cells from free radical damage brought on by the ischemia of chylomicron-induced changes in pancreatic capillary circulation.
Steroids (prednisolone 0.6 mg/kg/day and maintenance dose over 3 to 6 months) are indicated in autoimmune pancreatitis (AIP), characterized by infiltration of IgG4-positive plasma cells [74]. It is important to differentiate pancreatic cancer from AIP before starting steroid treatment and periodic analysis to be done to avoid steroid - induced pancreatic damage such as obstruction of small pancreatic ductules due to increased viscosity of pancreatic secretions.
The benefits of other agents such as antisecretory drugs (somatostatin, octreotide, lanreotide), N-acetyl cysteine and anti-inflammatory agent (lefipixant) are disappointing.
Surgical Therapy
Surgical intervention is associated with high risk of death than medical therapy especially in sterile pancreatitis. Documented infection has been considered as a definite indication for debridgement and infected necrosis may also be treated successfully with antibiotics alone.
A single- stage surgical transgastric necrosectomy is a good option in patients with disconnected pancreatic duct syndrome since it results peripancreatic collections in symptomatic patients with lack of improvement [75] and a postoperative mortality of 2% [76]. Routine intraoperative cholangiography is unnecessary in mild gallstone pancreatitis with normalizing bilirubin levels [77].
Interventional Therapy
A catheter directed balloon tamponade, coil embolization or covered stent is preferable to control the massive hemorrhage occurring in 1 to 3% of cases of severe acute pancreatitis and late hemorrhage due to rupture of pseudoaneurysm of splenic artery. Pancreatic duct stent placement may decrease the post ERCP pancreatitis in those patients undergoing endoscopic procedures such as ampullectomy.
Outcome
The disease takes a mild course in most patients and the severe form carries a hospital mortality rate of 15%. Infection occurs in 20-40% of cases, contribute to 80% of deaths in acute pancreatitis [78] and it is associated with worsening organ dysfunction in < 5% of cases. The mortality rate in patients with infected necrosis without organ failure is 1.4%. The mortality rate of sterile necrosis remains relatively low as 5 to 10% and without necrosis, it is 0% mortality [79], but the superinfection of necrosis increases the mortality rate subsequently up to 20 to 30% [80]. The sterile necrosis with organ failure is associated with a mortality rate of 19.8%. The treatment of damages caused by systemic inflammation and better antibiotic treatment, nutritional support and learned surgical decisions decrease both early (< 6 days due to SIRS) and late mortality [81].
Case Analysis
This 32 years old male was presented with acute abdomen as an initial manifestation of rheumatic fever due to Lancifield group A beta hemolytic streptococci [82] as evidenced by raised ASO titer and ESR. Elevated amylase and lipase with CT features of peripancreatic inflammatory changes as ‘mistiness’ (fat strandings) suggesting acute interstitial edematous pancreatitis (IEP) as in Figures 1 & 2 and these inflammatory changes are responded to antibiotic therapy. The patient improved dramatically within few days and resumed oral intake without any further complications. Cefotaxime showed good penetration into the pancreas to eradicate the infective process [83].
Presence of obesity, history of alcoholism, use of anticonvulsants and moderately raised triglyceride levels are the risk factors to trigger the pancreatic infection by streptococcus in this case. Periarteriolar connective tissue inflammation caused by the organism causes vasculitis and the resultant ischemia in the pancreas as an isolated event, may predisposes to further infection and so penicillin prophylaxis is indicated.
Preventive Measures
a) A healthy lifestyle can reduce the chances of developing acute pancreatitis.
Hypertriglyceridemia causes 2 to 5 % of cases of pancreatitis and is associated with inherited disorders of lipoprotein metabolism, congenital type1, II and V without a precipitating factor in children [84]. Chylomicrons are triglyceride-rich lipoprotein particles believed to be responsible for pancreatic inflammation. They usually present in the circulation when serum triglyceride levels exceed 10 mmol/L. These largest of lipoproteins might impair circulatory flow in capillary beds; if this occurs in the pancreas, the resulting ischemia might disturb the acinar structure and expose these triglyceride-rich particles to pancreatic lipase. The pro-inflammatory non-esterified free fatty acids generated from the enzymatic degradation of chylomicron-triglycerides (ie, the release of free fatty acids by lipase) may lead to further damage of pancreatic acinar cells and microvasculature. Subsequent amplification of the release of inflammatory mediators and free radicals may ultimately lead to necrosis, edema, and inflammation. Hypertriglyceridemia was the cause of 56% cases of gestational pancreatitis Mild to moderate elevations in triglycerides (2-10 mmol/L) are extremely common in the early phase of acute pancreatitis of any etiology. and more likely to be an epiphenomenon of the acute pancreatitis rather than a true causal precipitant. Triglyceride levels remained mildly elevated for up to 15 days, probably reflecting an underlying lipid disorder.
Fasting triglycerides >11.3 mmol/l (>1000 mg/dl) in convalescence suggests it as an etiological factor and alcohol itself increases the triglyceride level in a dose dependent manner and so avoidance of alcohol and reduction of triglyceride level are mandatory. In some cases, serum amylase levels may not be significantly elevated due to the interference from the triglycerides with certain amylase assays. Persistence of hyperlipidemia on a fat-reduced diet should prompt the institution of lipid-lowering agents. The fibric acid derivatives (fibrates), such as gemfibrozil, fenofibrate or bezafibrate, are the drugs of first choice. Omega-3 fatty-acid products show promise as adjunctive agents in refractory cases.
b) Prevention of infectious episodes
Overcrowding, environmental pollution, poor sanitary hygiene in public places (airports, railway stations, bus stands, markets, hotels, shopping areas, hospital premises, schools, household surroundings, streets, cinema theatres, roadsides & side of railway tracks, toilets in public places, smoke emitting and dust spreading vehicles on the roads) may prone to harbour the infections and the exposure of the mucosal surfaces (oral cavity, throat, nasopharynx, genitals) favour the entry of the organism into the body. Establishment of “public health units” in these places are advisable to identify symptomatic cases and to implement preventive measures.
Moreover, the patients may not adhere the lifelong penicillin prophylaxis to prevent its occurrence. The one-week course of “Pulse Therapy” as oral penicillin V (or penicillin G potassium tablets 400 mg daily), macrolides, cephalosporins and amoxicillin (amoxicillin should not be combined with penicillins) is advisable for each episode of attacks when the individual experiences sore throat, sneezing, running nose, febrile episodes with ASO titer positivity since silent and subclinical illness may cause organ damage via the immune mediated mechanisms [85].
Superinfection as Penicillin G potassium should not be used for extended periods since it can lead to the growth of dangerous organisms that are resistant or unresponsive to this medication.
New Insights
The systemic inflammatory response syndrome as “cytokine storm” plays a major role in the occurrence of acute pancreatitis and lung damage in streptococcus pyogene infection in susceptible patients. The ‘cytokine’ (bradykinin) storm is also responsible for ‘acute respiratory distress syndrome (ARDS)’ in COVID 19 patients and pancreatic involvement occurs in small number of affected individuals.
A ‘superantigen’ mediated acute infectious disease caused by human adapted pathogen group A streptococcus (GAS) and its large regional outbreaks emerged in North-East Asia in 2011, in United Kingdom in 2014 and the potential trigger for these epidemics remain unclear. Detailed phylogenetic analysis of GAS outbreak isolates from Mainland China and Hong Kong proved that the increase in fever cases were neither emm type specific nor caused by a single clone and the multiclonal fever outbreak strains are commonly associated with the acquisition of related exotoxin carrying mobile genetic elements [86].
Prophage encoding combination of streptococcal superantigens (SSA) and Spe (Streptococcal pyrogenic exotoxin) C, and Spd1 (streptococcal phage-encoded DNase), appear to play an important role in the evolutionary pathway that leads to emergence of more virulent strains [87-91]. GAS produces a cholesterol dependent cytolysin, the Streptolysin O (SLO), that perforates the host cell membrane and it directly damages the mucosa to allow the penetration of streptococcal pyrogenic exotoxin A (Spe A) [92], and Spe C and DNase Spd1 function synergistically to mediate nasopharyngeal colonization [93].
The superantigen, the most potent T cell mitogen known to date [94] and recent studies suggest that such T cell activation contributes to the establishment of GAS infection at mucosal surfaces [95,96]. The exotoxin genes SSa (streptococcal superantigen), Spe C and spd1 and their impact on exotoxin driven enhanced colonization provides an evidence-based hypothesis for the reemergence of infection globally similar to COVID 19 pandemic in which the pathogenic ACE 2 receptors are highly expressed in pancreatic islets although it’s clear mechanism is unknown.
The GAS cell surface bears M proteins that form short hair like fibrils. The key feature of M1 clone is it’s ability to switch rapidly to a hypervirulent phenotype during infection as a result of the CovR/S (cov, control of virulence; csrRS), two component system, a global regulator of virulence gene expression in GAS. GAS posses a large battery of virulence factors, trigger the potent inflammatory response, leading to streptococcal toxic shock syndrome with multiorgan dysfunction, vascular collapse, and death in genetically susceptible individuals. GAS causes community acquired pneumonia in 2 to 5% of cases, most commonly after the outbreaks of viral illnesses such as influenza or measles. The current upsurge of invasive infection in developed countries is predominantly linked to the spread of clonal hypervirulent population of M1T1 serotype strain, also seen with M3 and M18 strain, which co-emerged with M1T1 clonal strain and M59 in Western provinces. The new clones evolve through the accumulation of point mutations or by acquisition of new genetic material through horizontal gene transfer events.
GAS can be transmitted by direct or indirect contact and by droplets similar to SARS-Cov-2. Health care workers may be the source of transmission to secondary nosocomial cases. Epidemiologically, specimens from mucosal surfaces, the nasopharynx, genitals (vagina) and anus for cultures, and the positive cases should be treated with antibiotics in order to eradicate the GAS infection.
The persons > 65 years are at increased risk of sporadic cases or mortality due to GAS infection [97]. For asymptomatic group A streptococcal colonized health care workers, benzathine penicillin G 12 lakhs IM + rifampin 300 mg twice daily for 4 days, clindamycin 300mg orally three times a day for 10 days or azithromycin 500 mg orally daily for 5 days are advised. Rectal carriage of GAS are difficult to eradicate with penicillin based regimens. Oral therapy with vancomycin and rifampin has been recommended and Clindamycin is the preferred agent in such cases since it has documented effects on intestinal flora.
Future Directions
1.Immunoneutralization
In GAS infection, M-protein reactive T cells enter through the surface endothelium by binding to cell adhesion molecules such as VCAM 1(vascular cell adhesion molecule 1), causing leukocyte activation and compromise blood oxygenation [98] by massive release of cytokines as noticed in COVID 19.
Immune neutralization of these specific adhesion molecules (ICAM 1 (intercellular adhesion molecule 1), Mac 1 (macrophage-1 antigen), LFA 1(lymphocyte function–associated antigen 1) and PSGL 1(P-selectin glycoprotein ligand-1)) decrease the neutrophil infiltration and ameliorate the endotoxemia, acute lung damage and pancreatic inflammation [99,100].
2.Immunomodulation
Stem cell therapy
Mesenchymal stem cell therapy (MSCs) reduces the serum levels of proinflammatory cytokines (TNF-α, IFN-γ, IL-1β and IL-6) and decrease the acute inflammatory response via their immunomodulatory effect by secreting anti-inflammatory cytokines (IL-4, IL-10). Umbilical cord derived mesenchymal stem cells injection exerts the degenerative effect of damaged pancreatic cells via a paracrine immunosuppressive effect rather than by directly differentiating into tissue- specific pancreatic cells, antiapoptotic effect by secreting the chemokine XCL 1, suppress CD4+T cell proliferation [101] in the development of tissue injury during acute pancreatitis and enhancing angiogenesis. The SDF/CXCR 4 axis (Stromal cell-derived factor/CXCR4 chemokine receptor) [102] regulate the migration of mesenchymal stem cells following acute pancreatitis by upregulating the SDF1 in the injured pancreas when most intravenously infused MSCs become trapped in the lungs. It downregulates the expression of TGF-β1 (Transforming growth factor beta 1), which is a major regulator of chronic inflammation and fibrosis and attenuate the local hypoxia and oxidative stress. It suppress T cell proliferation and B cell maturation and activate the regulatory T cells to further suppress the immune response. Since the first 24 hours after the onset of acute pancreatitis is critical for prognosis, only a few studies evaluated the outcome of MSCs [103,104] as an attractive source of cell therapy. Within this time frame, it is a current conservative therapy to reduce mortality by ameliorating the acute process of pancreatic inflammation.
Icariin is a flavonoid with rhamnose as a ligand, a traditional Chinese medicine, extracted from potent Horny Goat Weed [105]. It acts as a natural anti-inflammatory drug which targets on proinflammatory cytokines (TNF-α, IL-6) and activate phosphoinositol 3 - kinase (PI3K) protein kinase B (AKT) signaling pathway to ameliorate lipopolysaccharide (LPS)-induced acute inflammatory responses [106]. It has potent antioxidant activity and eliminate the reactive oxygen species (ROS). It preserves the proliferative power of MSCs and decrease their senescence and dysfunction. It acts as a preconditioning agent that increases the paracrine activity of MSCs. MSCs co-transplanted with Icariin improves the function of pancreatic stellate cells by enhancing the key β-cell markers PDX1 (pancreatic and duodenal homeobox factor 1) and MafA (musculoaponeurotic fibrosarcoma oncogene homolog A).
C1 esterase inhibitor stabilizes the intravascular fluid status and prevent multiorgan failure caused by inflammatory chemokine MCP-1(Monocyte chemoattractant protein-1) and FKN (Fractalkine) and prevent the development of acute pancreatitis following allogenic hematopoietic stem cell transplantation due to complement activation. Complement activation such as capillary leakage syndrome [107] plays a central role in mediating the systemic effects of acute pancreatitis. C1 esterase inhibitor reverses the cardiovascular instability and acute renal failure resulting from third spacing of fluids and resolution of serous effusion, but not significantly influences the local inflammation and autodigestive destruction of pancreas [108] due to self perpetuating activation of protease enzymes.
Aprotinin, a kunitz protease inhibitor, has inhibitory activity against trypsin, chymotrypsin, kallikrein and when given intraperitoneally in high doses, it counteracts the development of necrosis in patients with severe acute pancreatitis [109,110].
Use of immunomodulating agents such as IV polyspecific Immunoglobulin G (IV IG) that neutralize the toxins and pathological levels of pro-inflammatory cytokines are beneficial.
3. PCR test
Identification of serum opacity factor (sof) gene which serves as a marker for serotyping of streptococcus pyogenes. Sof binds to fibulin 1 and fibrinogen present in the serum and it is a bifunctional cell surface protein expressed by 40 to 50% of group A streptococcal strain composed of C terminal domain that binds fibronectin and an N terminal domain that mediates opacification of mammalian sera. It exhibits N terminal sequence variation and is under the positive transcriptional variation of mga (multiple gene activator) and elicits type specific immune response [111]. Sof is a unique virulence gene of streptococcus pyogenes and plays an important role in fibulin binding, opacifying the serum and adhesion of pathogen to the epithelial cells of the host [112].
PCR (polymerase chain reaction) is a powerful tool in detection of streptococcus pyogenes in 1 hour without isolating genomic DNA from the pathogen. Sof is a virulence gene and does not have homology with other organisms and it can be used as a genetic marker for the detection of streptococcus pyogenes causing pharyngitis, pancreatitis and ARDS (acute respiratory distress syndrome).
Conclusion
GAS pharngitis and invasive infections are more common as seasonal trends, “a wave of airborne infection” with close ‘person-to-person contacts’ and predisposing to viral infections [113]. Mucosal hygiene (nasal, oral cavity and genitals) is an important measure to prevent it [114]. COVID 19 is similarly presenting and amenable to antibiotics in mild cases and vaccine development remains as a challenge for both conditions since seroconversions occurring frequently as noticed in the United Kingdom due to new outbreaks of corona virus with different strains recently. Live attenuated vaccine similar to oral polio vaccine as “drops” at the exposed mucosal surfaces of the body (mucosal vaccine) to induce immunity (both ‘humoral’ or serum immunity and local immune response) is a better option to control the outbreaks.
Acute abdomen, as pancreatitis and acute lung damage, as ARDS are the presenting manifestations of both of these infections. Penicillin prophylaxis is indicated in endemic areas to prevent it’s unexpected outbreaks and, serum ASO titer screening and PCR tests are advised to identify these infections.
References
- Johnson, C.D., Besselink, M., G.,Carter,R.(2014) Acute Pancreatitis, British Medical Journal, 349, g 4859.
- Goldacre, Michael J., and Stephen E. Roberts. "Hospital admission for acute pancreatitis in an English population, 1963- 98: database study of incidence and mortality." Bmj 328, no. 7454 (2004): 1466-1469.
- Rebours, Vinciane, Marie-Pierre Vullierme, Olivia Hentic, Frédérique Maire, Pascal Hammel, Philippe Ruszniewski, and Philippe Lévy. "Smoking and the course of recurrent acute and chronic alcoholic pancreatitis: a dose-dependent relationship." Pancreas 41, no. 8 (2012): 1219-1224.
- Whitcomb, David C. "Genetic polymorphisms in alcoholic pancreatitis." Digestive Diseases 23, no. 3-4 (2006): 247-254.
- Isenmann, Rainer, Michael Rünzi, Martina Kron, Stefan Kahl, Dietmar Kraus, Norbert Jung, Ludwig Maier, Peter Malfertheiner, Harald Goebell, and Hans G. Beger. "Prophylactic antibiotic treatment in patients with predicted severe acute pancreatitis: a placebo-controlled, double-blind trial." Gastroenterology 126, no. 4 (2004): 997-1004.
- Picard, E., A. Gedalia, P. Benmeir, N. Zucker, and Y. Barki. "Abdominal pain with free peritoneal fluid detected by ultrasonography as a presenting manifestation of acute rheumatic fever." Annals of the rheumatic diseases 51, no. 3 (1992): 394-395.
- Hogan, W. J., J. E. Geenen, and W. J. Dodds. "Dysmotility disturbances of the biliary tract: classification, diagnosis, and treatment." In Seminars in liver disease, vol. 7, no. 04, pp. 302- 310. © 1987 by Thieme Medical Publishers, Inc., 1987.
- Beger, Hans G., and Bettina M. Rau. "Severe acute pancreatitis: clinical course and management." World journal of gastroenterology: WJG 13, no. 38 (2007): 5043.
- Perez, Alexander, Edward E. Whang, David C. Brooks, Francis D. Moore Jr, Michael D. Hughes, Gregory T. Sica, Michael J. Zinner, Stanley W. Ashley, and Peter A. Banks. "Is severity of necrotizing pancreatitis increased in extended necrosis and infected necrosis?." Pancreas 25, no. 3 (2002): 229-233.
- Mourad, M. M., R. P. T. Evans, V. Kalidindi, R. Navaratnam, L. Dvorkin, and S. R. Bramhall. "Prophylactic antibiotics in acute pancreatitis: endless debate." The Annals of The Royal College of Surgeons of England 99, no. 2 (2017): 107-112.
- Reuken, Philipp A., Hanna Albig, Jürgen Rödel, Michael Hocke, Uwe Will, Andreas Stallmach, and Tony Bruns. "Fungal infections in patients with infected pancreatic necrosis and pseudocysts: risk factors and outcome." Pancreas 47, no. 1 (2018): 92-98.
- Chiu, Cheng-Hsun, Tzou-Yien Lin, and Jue-Lan Wu. "Acute pancreatitis associated with streptococcal toxic shock syndrome." Clinical infectious diseases 22, no. 4 (1996): 724-726.
- Liu, Furong, Xin Long, Bixiang Zhang, Wanguang Zhang, Xiaoping Chen, and Zhanguo Zhang. "ACE2 expression in pancreas may cause pancreatic damage after SARS-CoV-2 infection." Clinical Gastroenterology and Hepatology 18, no. 9 (2020): 2128.
- Wang, F.,Wang,H.,Fan,J.,(2020)Pancreatic Injury Patterns In Patients With Corona virus Disease 19 Pneumonia, Gastroenterology, 159, 367-370..
- Aloysius, Mark M., Ashwin Thatti, Anjalika Gupta, Nishant Sharma, Pardeep Bansal, and Hemant Goyal. "COVID-19 presenting as acute pancreatitis." Pancreatology 20, no. 5 (2020): 1026-1027.
- Anand, E. R., C. Major, O. Pickering, and M. Nelson. "Acute pancreatitis in a COVID-19 patient." Journal of British Surgery 107, no. 7 (2020): e182-e182.
- Kandasamy, Sathish. "An unusual presentation of COVID-19: acute pancreatitis." Annals of Hepato-biliary-pancreatic Surgery 24, no. 4 (2020): 539-541.
- Bradley, Edward L. "A clinically based classification system for acute pancreatitis: summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992." Archives of surgery 128, no. 5 (1993): 586-590.
- Besselink, Marc GH, Hjalmar C. van Santvoort, Ben J. Witteman, Hein G. Gooszen, and Dutch Acute Pancreatitis Study Group. "Management of severe acute pancreatitis: it's all about timing." Current opinion in critical care 13, no. 2 (2007): 200- 206.
- Johnson, C. D., and M. Abu-Hilal. "Persistent organ failure during the first week as a marker of fatal outcome in acute pancreatitis." Gut 53, no. 9 (2004): 1340-1344.
- Abu-Zidan, F. M., M. J. D. Bonham, and J. A. Windsor. "Severity of acute pancreatitis: a multivariate analysis of oxidative stress markers and modified Glasgow criteria." Journal of British Surgery 87, no. 8 (2000): 1019-1023.
- Toouli, James, Mark Brooke-Smith, Claudio Bassi, D. Carr- Locke, J. Telford, P. Freeny, C. Imrie, and R. Tandon. "Guidelines for the management of acute pancreatitis." Journal of Gastroenterology & Hepatology 17 (2002).
- Tenner, S., J. Baillie, J. DeWitt, and S. S. Vege. "American College of Gastroenterology guideline: Management of acute pancreatitis. American College of Gastroenterology." Am. J. Gastroenterol 108, no. 9 (2013): 1400-1416.
- Rompianesi, Gianluca, Angus Hann, Oluyemi Komolafe, Stephen P. Pereira, Brian R. Davidson, and Kurinchi Selvan Gurusamy. "Serum amylase and lipase and urinary trypsinogen and amylase for diagnosis of acute pancreatitis." Cochrane Database of Systematic Reviews 4 (2017).
- Matull, W. R., S. P. Pereira, and J. W. O’donohue. "Biochemical markers of acute pancreatitis." Journal of clinical pathology 59, no. 4 (2006): 340-344.
- Chang, Kai, Weiping Lu, Kejun Zhang, Shuangrong Jia, Fake Li, Feng Wang, Shaoli Deng, and Ming Chen. "Rapid urinary trypsinogen-2 test in the early diagnosis of acute pancreatitis: a meta-analysis." Clinical biochemistry 45, no. 13-14 (2012): 1051-1056.
- Staubli, Sebastian Manuel, Daniel Oertli, and Christian Andreas Nebiker. "Laboratory markers predicting severity of acute pancreatitis." Critical reviews in clinical laboratory sciences 52, no. 6 (2015): 273-283.
- Kibar, Yunus İ., Fatih Albayrak, Mahmut Arabul, Hakan Dursun, Yavuz Albayrak, and Yasin Ozturk. "Resistin: new serum marker for predicting severity of acute pancreatitis." Journal of International Medical Research 44, no. 2 (2016): 328-337.
- Yu, Pengfei, Shiqi Wang, Zhaoyan Qiu, Bin Bai, Zhanwei Zhao, Yiming Hao, Qian Wang et al. "Efficacy of resistin and leptin in predicting persistent organ failure in patients with acute pancreatitis." Pancreatology 16, no. 6 (2016): 952-957.
- Assicot, Marcel, C. Bohuon, D. Gendrel, Josette Raymond, H. Carsin, and J. J. T. L. Guilbaud. "High serum procalcitonin concentrations in patients with sepsis and infection." The Lancet 341, no. 8844 (1993): 515-518.
- Yang, Catherine J., Joseph Chen, Anthony RJ Phillips, John A. Windsor, and Maxim S. Petrov. "Predictors of severe and critical acute pancreatitis: a systematic review." Digestive and Liver Disease 46, no. 5 (2014): 446-451.
- Chang, Lin, Simon K. Lo, Bruce E. Stabile, Roger J. Lewis, and Christian De Virgilio. "Gallstone pancreatitis: a prospective study on the incidence of cholangitis and clinical predictors of retained common bile duct stones." Official journal of the American College of Gastroenterology| ACG 93, no. 4 (1998): 527-531.
- Cho, Joon Hyun, Tae Nyeun Kim, Hyun Hee Chung, and Kook Hyun Kim. "Comparison of scoring systems in predicting the severity of acute pancreatitis." World journal of gastroenterology: WJG 21, no. 8 (2015): 2387.
- Wu, Bechien U., Richard S. Johannes, Xiaowu Sun, Ying Tabak, Darwin L. Conwell, and Peter A. Banks. "The early prediction of mortality in acute pancreatitis: a large population-based study." Gut 57, no. 12 (2008): 1698-1703.
- Park, Ji Young, Tae Joo Jeon, Tae Hwan Ha, Jin Tae Hwang, Dong Hyun Sinn, Tae-Hoon Oh, Won Chang Shin, and Won- Choong Choi. "Bedside index for severity in acute pancreatitis: comparison with other scoring systems in predicting severity and organ failure." Hepatobiliary & Pancreatic Diseases International 12, no. 6 (2013): 645-650.
- Baron, Todd H. "Managing severe acute pancreatitis." Cleveland Clinic journal of medicine 80, no. 6 (2013): 354-359.
- Chakraborty, Rebanta K., and Bracken Burns. "Systemic inflammatory response syndrome." (2019).
- Kim, Young Kon, Seog Wan Ko, Chong Soo Kim, and Seung Bae Hwang. "Effectiveness of MR imaging for diagnosing the mild forms of acute pancreatitis: comparison with MDCT." Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine 24, no. 6 (2006): 1342-1349.
- Balthazar, Emil J., David L. Robinson, Alec J. Megibow, and J. H. Ranson. "Acute pancreatitis: value of CT in establishing prognosis." Radiology 174, no. 2 (1990): 331-336.
- Bollen, Thomas L., Vikesh K. Singh, Rie Maurer, Kathryn Repas, Hendrik W. Van Es, Peter A. Banks, and Koenraad J. Mortele. "Comparative evaluation of the modified CT severity index and CT severity index in assessing severity of acute pancreatitis." American Journal of Roentgenology 197, no. 2 (2011): 386-392.
- Balthazar, Emil J. "Acute pancreatitis: assessment of severity with clinical and CT evaluation." Radiology 223, no. 3 (2002): 603-613.
- Giljaca,V.,Gurusamy,K.,S.,Takwoingi,Y.,Higgie,D.,Poropat, G.,Stimac,D.,et. al (2015) Endoscopic Ultrasound Versus Magnetic Resonance Cholangiopancreatography For Common Bile Duct Stones, Cochrane Data Base Systematic Reviews, 2, CD011549.
- Sharma, Malay, Amit Pathak, Chittapuram Srinivasan Rameshbabu, Praveer Rai, Vijendra Kirnake, and Abid Shoukat. "Imaging of pancreas divisum by linear-array endoscopic ultrasonography." Endoscopic ultrasound 5, no. 1 (2016): 21-29.
- Byrne, Michael F., and Paul S. Jowell. "Gastrointestinal imaging: endoscopic ultrasound." Gastroenterology 122, no. 6 (2002): 1631-1648.
- Xiao, Bo, Xiao-Ming Zhang, Wei Tang, Nan-Lin Zeng, and Zhao-Hua Zhai. "Magnetic resonance imaging for local complications of acute pancreatitis: a pictorial review." World Journal Of Gastroenterology: WJG 16, no. 22 (2010): 2735.
- Tse, Frances, and Yuhong Yuan. "Early routine endoscopic retrograde cholangiopancreatography strategy versus early conservative management strategy in acute gallstone pancreatitis." Cochrane database of systematic reviews 5 (2012).
- Hurter, Delmé, Coert De Vries, Pierre Potgieter, Renald Barry, Frikkie Botha, and Gina Joubert. "Accuracy of MRCP compared to ERCP in the diagnosis of bile duct disorders." SA Journal of Radiology 12, no. 1 (2008): 14-22.
- Yattoo, G. N., Waiz Gowhar Amin, Feroze A. Shaheen, Showkat Zargar, and Gul Javid. "The efficacy of magnetic resonance cholangiopancreatography in assessing the etiology of acute idiopathic pancreatitis." Int J Hepatobiliary Pancreat Dis 4 (2014): 32-39.
- Manfredi, Riccardo, and Roberto Pozzi Mucelli. "Secretin-enhanced MR imaging of the pancreas." Radiology 279, no. 1 (2016): 29-43.
- Banks, P., A., Freeman, M.,L.,(2006) Practice Guidelines In Acute Pancreatitis. American Journal of Gastroenterology, 101, 2379–2400.
- Eckerwall, Gunilla E., Bobby BÅ Tingstedt, Per E. Bergenzaun, and Roland G. Andersson. "Immediate oral feeding in patients with mild acute pancreatitis is safe and may accelerate recovery— a randomized clinical study." Clinical nutrition 26, no. 6 (2007): 758-763.
- Takeda, Kazunori, Yukio Mikami, Shoji Fukuyama, Shinichi Egawa, Makoto Sunamura, Tadashi Ishibashi, Akihiro Sato, Atsushi Masamune, and Seiki Matsuno. "Pancreatic ischemia associated with vasospasm in the early phase of human acute necrotizing pancreatitis." Pancreas 30, no. 1 (2005): 40-49.
- Fisher, Jessica M., and Timothy B. Gardner. "The “golden hours” of management in acute pancreatitis." Official journal of the American College of Gastroenterology| ACG 107, no. 8 (2012): 1146-1150.
- Gardner, Timothy B., Santhi Swaroop Vege, Randall K. Pearson, and Suresh T. Chari. "Fluid resuscitation in acute pancreatitis." Clinical Gastroenterology and Hepatology 6, no. 10 (2008): 1070-1076.
- Wu, Bechien U., James Q. Hwang, Timothy H. Gardner, Kathryn Repas, Ryan Delee, Song Yu, Benjamin Smith, Peter A. Banks, and Darwin L. Conwell. "Lactated Ringer's solution reduces systemic inflammation compared with saline in patients with acute pancreatitis." Clinical Gastroenterology and Hepatology 9, no. 8 (2011): 710-717.
- Mao, En-qiang, Jian Fei, Yi-bing Peng, Jie Huang, Yao-qing Tang, and Sheng-dao Zhang. "Rapid hemodilution is associated with increased sepsis and mortality among patients with severe acute pancreatitis." Chinese medical journal 123, no. 13 (2010): 1639-1644.
- de-Madaria, Enrique, Gema Soler-Sala, José Sánchez-Payá, Inmaculada Lopez-Font, Juan Martínez, Laura Gómez-Escolar, Laura Sempere, Cristina Sánchez-Fortún, and Miguel Pérez-Mateo. "Influence of fluid therapy on the prognosis of acute pancreatitis: a prospective cohort study." Official journal of the American College of Gastroenterology| ACG 106, no. 10 (2011): 1843-1850.
- Eckerwall, Gunilla, Hanna Olin, Bodil Andersson, and Roland Andersson. "Fluid resuscitation and nutritional support during severe acute pancreatitis in the past: what have we learned and how can we do better?." Clinical nutrition 25, no. 3 (2006): 497-504.
- Windsor, A. C. J., S. Kanwar, A. G. K. Li, E. Barnes, J. A. Guthrie, J. I. Spark, F. Welsh, P. J. Guillou, and J. V. Reynolds. "Compared with parenteral nutrition, enteral feeding attenuates the acute phase response and improves disease severity in acute pancreatitis." Gut 42, no. 3 (1998): 431-435.
- Bakker, Olaf J., Sandra van Brunschot, Hjalmar C. van Santvoort, Marc G. Besselink, Thomas L. Bollen, Marja A. Boermeester, Cornelis H. Dejong et al. "Early versus on-demand nasoenteric tube feeding in acute pancreatitis." New England Journal of Medicine 371, no. 21 (2014): 1983-1993.
- Eatock, F. C., P. Chong, N. Menezes, L. Murray, C. J. McKay, C. R. Carter, and C. W. Imrie. "A randomized study of early nasogastric versus nasojejunal feeding in severe acute pancreatitis." Official journal of the American College of Gastroenterology| ACG 100, no. 2 (2005): 432-439.
- Pederzoli, Paolo, Claudio Bassi, Sergio Vesentini, and Angelo Campedelli. "A randomized multicenter clinical trial of antibiotic prophylaxis of septic complications in acute necrotizing pancreatitis with imipenem." Surgery, gynecology & obstetrics 176, no. 5 (1993): 480-483.
- Jiang, Kun, Wei Huang, Xiao-Nan Yang, and Qing Xia. "Present and future of prophylactic antibiotics for severe acute pancreatitis." World journal of gastroenterology: WJG 18, no. 3 (2012): 279.
- Schmid, S. W., W. Uhl, H. Friess, P. Malfertheiner, and M. W. Büchler. "The role of infection in acute pancreatitis." Gut 45, no. 2 (1999): 311-311.
- De Waele, Jan J. "Rational use of antimicrobials in patients with severe acute pancreatitis." In Seminars in respiratory and critical care medicine, vol. 32, no. 02, pp. 174-180. © Thieme Medical Publishers, 2011.
- Eloubeidi, Mohamad A., Ashutosh Tamhane, Shyam Varadarajulu, and C. Mel Wilcox. "Frequency of major complications after EUS-guided FNA of solid pancreatic masses: a prospective evaluation." Gastrointestinal endoscopy 63, no. 4 (2006): 622-629.
- Nathens, Avery B., J. Randall Curtis, Richard J. Beale, Deborah J. Cook, Rui P. Moreno, Jacques-Andre Romand, Shawn J. Skerrett, Renee D. Stapleton, Lorraine B. Ware, and Carl S. Waldmann. "Management of the critically ill patient with severe acute pancreatitis." Critical care medicine 32, no. 12 (2004): 2524-2536.
- Büchler, Markus, Peter Malfertheiner, Helmut Frieβ, Rainer Isenmann, Ernst Vanek, Heinz Grimm, Paul Schlegel, Thomas Friess, and Hans G. Beger. "Human pancreatic tissue concentration of bactericidal antibiotics." Gastroenterology 103, no. 6 (1992): 1902-1908.
- Otto, W., K. Komorzycki, and M. Krawczyk. "Efficacy of antibiotic penetration into pancreatic necrosis." Hpb 8, no. 1 (2006): 43-48.
- Schubert, Sabine, and Axel Dalhoff. "Activity of moxifloxacin, imipenem, and ertapenem against Escherichia coli, Enterobacter cloacae, Enterococcus faecalis, and Bacteroides fragilis in monocultures and mixed cultures in an in vitro pharmacokinetic/ pharmacodynamic model simulating concentrations in the human pancreas." Antimicrobial agents and chemotherapy 56, no. 12 (2012): 6434-6436.
- Li, J., T. R. Chen, H. L. Gong, M. H. Wan, G. Y. Chen, and W. F. Tang. "Intensive insulin therapy in severe acute pancreatitis: a meta-analysis and systematic review." West Indian Med J 61, no. 6 (2012): 574-579.
- Stefanutti, Claudia, Giancarlo Labbadia, and Claudia Morozzi. "Severe hypertriglyceridemia-related acute pancreatitis." Therapeutic Apheresis and Dialysis 17, no. 2 (2013): 130-137.
- He, Chaosheng, Li Zhang, Wei Shi, Xinling Liang, Zhiming Ye, Bin Zhang, and Shuangxin Liu. "Coupled plasma filtration adsorption combined with continuous veno-venous hemofiltration treatment in patients with severe acute pancreatitis." Journal of clinical gastroenterology 47, no. 1 (2013): 62-68.
- Pannala, Rahul, and Suresh T. Chari. "Corticosteroid treatment for autoimmune pancreatitis." Gut 58, no. 11 (2009): 1438- 1439.
- Dua, Monica M., Christopher W. Jensen, Shai Friedland, Patrick J. Worth, George A. Poultsides, Jeffrey A. Norton, Walter G. Park, and Brendan C. Visser. "Isolated pancreatic tail remnants after transgastric necrosectomy can be observed." Journal of Surgical Research 231 (2018): 109-115.
- Bang, Ji Young, Charles Melbern Wilcox, Udayakumar Navaneethan, Muhammad K. Hasan, Shajan Peter, John Christein, Robert Hawes, and Shyam Varadarajulu. "Impact of disconnected pancreatic duct syndrome on the endoscopic management of pancreatic fluid collections." Annals of Surgery 267, no. 3 (2018): 561-568.
- Pham, Xuan-Binh D., Christian de Virgilio, Lutfi Al-Khouja, Michael C. Bermudez, Alexander C. Schwed, Amy H. Kaji, David S. Plurad et al. "Routine intraoperative cholangiography is unnecessary in patients with mild gallstone pancreatitis and normalizing bilirubin levels." The American Journal of Surgery 212, no. 6 (2016): 1047-1053.
- Delcenserie, R., T. Yzet, and J. P. Ducroix. "Prophylactic antibiotics in treatment of severe acute alcoholic pancreatitis." Pancreas 13, no. 2 (1996): 198-201.
- Mann, D. V., M. J. Hershman, R. Hittinger, and G. Glazer. "Multicentre audit of death from acute pancreatitis." Journal of British Surgery 81, no. 6 (1994): 890-893.
- IAP, Working Group, and APA Acute Pancreatitis Guidelines. "IAP/APA evidence-based guidelines for the management of acute pancreatitis." Pancreatology 13, no. 4 (2013): e1-e15.
- Wyncoll, D. L. "The management of severe acute necrotising pancreatitis: an evidence-based review of the literature." Intensive care medicine 25, no. 2 (1999): 146.
- Cross, H. D. "Pancreatitis and acute rheumatic fever." The Journal of the Maine Medical Association 56, no. 12 (1965): 268-268.
- https://www.mediresonline.org/journals/journal-of-dental-and-oral-care/article/action-of-a-cleaning-agent-on-saliva-contaminated-zirconia-study-by-nuclear-magnetic-resonance-spectroscopy-and-energy-dispersive-x-ray-microanalysis
- Murphy, M.,J.,Sheng,X., MacDonald, T.,Wei,L.,(2012) Hypertriglyceridemia And Acute Pancreatitis, Archives of Internal Medicine, 173, 1-3.
- Ramachandran (2019) Occupational Health- Mineralization of Heart Valves, 2nd Global Summit On Occupational Health & Safety, Dubai-Deira (Crowne Plaza), October, 11-12 (You Tube).
- You, Yuanhai, Mark R. Davies, Melinda Protani, Liam McIntyre, Mark J. Walker, and Jianzhong Zhang. "Scarlet fever epidemic in China caused by Streptococcus pyogenes serotype M12: epidemiologic and molecular analysis." EBioMedicine 28 (2018): 128-135.
- Tse, Herman, Jessie YJ Bao, Mark R. Davies, Peter Maamary, Hoi-Wah Tsoi, Amy HY Tong, Tom CC Ho et al. "Molecular characterization of the 2011 Hong Kong scarlet fever outbreak." The Journal of infectious diseases 206, no. 3 (2012): 341-351.
- Turner, Claire E., Marta Pyzio, Bonita Song, Theresa Lamagni, Margie Meltzer, J. Yimmy Chow, Androulla Efstratiou, Sally Curtis, and Shiranee Sriskandan. "Scarlet fever upsurge in England and molecular-genetic analysis in North-West London, 2014." Emerging infectious diseases 22, no. 6 (2016): 1075.
- Chalker, Victoria, Aleksey Jironkin, Juliana Coelho, Ali Al-Shahib, Steve Platt, Georgia Kapatai, Roger Daniel et al. "Genome analysis following a national increase in scarlet fever in England 2014." BMC genomics 18 (2017): 1-10.
- Davies, Mark R., Matthew T. Holden, Paul Coupland, Jonathan HK Chen, Carola Venturini, Timothy C. Barnett, Nouri L. Ben Zakour et al. "Emergence of scarlet fever Streptococcus pyogenes emm 12 clones in Hong Kong is associated with toxin acquisition and multidrug resistance." Nature genetics 47, no. 1 (2015): 84-87.
- Silva-Costa, Catarina, Joao A. Carriço, Mario Ramirez, and Jose Melo-Cristino. "Scarlet fever is caused by a limited number of Streptococcus pyogenes lineages and is associated with the exotoxin genes ssa, speA and speC." The Pediatric infectious disease journal 33, no. 3 (2014): 306-310.
- Brosnahan, Amanda J., Mary J. Mantz, Christopher A. Squier, Marnie L. Peterson, and Patrick M. Schlievert. "Cytolysins augment superantigen penetration of stratified mucosa." The Journal of Immunology 182, no. 4 (2009): 2364-2373.
- Broudy, Thomas B., Vijaykumar Pancholi, and Vincent A. Fischetti. "The in vitro interaction of Streptococcus pyogenes with human pharyngeal cells induces a phage-encoded extracellular DNase." Infection and immunity 70, no. 6 (2002): 2805- 2811
- Lamagni, Theresa, Rebecca Guy, Meera Chand, Katherine L. Henderson, Victoria Chalker, James Lewis, Vanessa Saliba et al. "Resurgence of scarlet fever in England, 2014–16: a population- based surveillance study." The Lancet Infectious Diseases 18, no. 2 (2018): 180-187.
- Kasper, Katherine J., Joseph J. Zeppa, Adrienne T. Wakabayashi, Stacey X. Xu, Delfina M. Mazzuca, Ian Welch, Miren L. Baroja et al. "Bacterial superantigens promote acute nasopharyngeal infection by Streptococcus pyogenes in a human MHC Class II-dependent manner." PLoS pathogens 10, no. 5 (2014): e1004155.
- Zeppa, Joseph J., Katherine J. Kasper, Ivor Mohorovic, Delfina M. Mazzuca, SM Mansour Haeryfar, and John K. McCormick. "Nasopharyngeal infection by Streptococcus pyogenes requires superantigen-responsive Vβ-specific T cells." Proceedings of the National Academy of Sciences 114, no. 38 (2017): 10226-10231.
- Brouwer, Stephan, Timothy C. Barnett, Diane Ly, Katherine J. Kasper, David MP De Oliveira, Tania Rivera-Hernandez, Amanda J. Cork et al. "Prophage exotoxins enhance colonization fitness in epidemic scarlet fever-causing Streptococcus pyogenes." Nature communications 11, no. 1 (2020): 5018.
- https://www.scirp.org/journal/paperinformation?paperid=85436
- Herwald, Heiko, Henning Cramer, Matthias Mörgelin, Wayne Russell, Ulla Sollenberg, Anna Norrby-Teglund, Hans Flodgaard, Lennart Lindbom, and Lars Björck. "M protein, a classical bacterial virulence determinant, forms complexes with fibrinogen that induce vascular leakage." Cell 116, no. 3 (2004): 367-379.
- Menezes, Gustavo Batista, Woo-Yong Lee, Hong Zhou, Christopher Curtis Matchett Waterhouse, Denise Carmona Cara, and Paul Kubes. "Selective down-regulation of neutrophil Mac- 1 in endotoxemic hepatic microcirculation via IL-10." The Journal of Immunology 183, no. 11 (2009): 7557-7568.
- Duffy, Michelle M., Thomas Ritter, Rhodri Ceredig, and Matthew D. Griffin. "Mesenchymal stem cell effects on T-cell effector pathways." Stem cell research & therapy 2 (2011): 1-9.
- Gong, Jian, Hong-Bo Meng, Jie Hua, Zhen-Shun Song, Zhi- Gang He, Bo Zhou, and Ming-Ping Qian. "The SDF-1/CXCR4 axis regulates migration of transplanted bone marrow mesenchymal stem cells towards the pancreas in rats with acute pancreatitis." Molecular medicine reports 9, no. 5 (2014): 1575- 1582.
- Yang, Bin, Bin Bai, Chao-Xu Liu, Shi-Qi Wang, Xue Jiang, Cai- Lin Zhu, and Qing-Chuan Zhao. "Effect of umbilical cord mesenchymal stem cells on treatment of severe acute pancreatitis in rats." Cytotherapy 15, no. 2 (2013): 154-162.
- He, Zhigang, Jie Hua, Daohai Qian, Jian Gong, Shengping Lin, Chenglei Xu, Ge Wei et al. "Intravenous hMSCs ameliorate acute pancreatitis in mice via secretion of tumor necrosis factor-α stimulated gene/protein 6." Scientific Reports 6, no. 1 (2016): 38438.
- Fang, Jian, and Yongjun Zhang. "Icariin, an anti-atherosclerotic drug from Chinese medicinal herb horny goat weed." Frontiers in pharmacology 8 (2017): 734.
- Xu, Chang-Qing, Bao-Jun Liu, Jin-Feng Wu, Yan-Chun Xu, Xiao-Hong Duan, Yu-Xue Cao, and Jing-Cheng Dong. "Icariin attenuates LPS-induced acute inflammatory responses: Involvement of PI3K/Akt and NF-κB signaling pathway." European journal of pharmacology 642, no. 1-3 (2010): 146-153.
- Nürnberger, W., Ruth Heying, S. Burdach, and U. Göbel. "C1 esterase inhibitor concentrate for capillary leakage syndrome following bone marrow transplantation." Annals of hematology 75 (1997): 95-101.
- Schneider, D. T., W. Nürnberger, H. Stannigel, H. Bönig, and U. Göbel. "Adjuvant treatment of severe acute pancreatitis with C1 esterase inhibitor concentrate after haematopoietic stem cell transplantation." Gut 45, no. 5 (1999): 733-736.
- Smith, M., H. M. Kocher, and B. J. Hunt. "Aprotinin in severe acute pancreatitis." International journal of clinical practice 64, no. 1 (2010): 84-92.
- Berling, Rikard, Sven Genell, and Kjell Ohlsson. "High-dose intraperitoneal aprotinin treatment of acute severe pancreatitis: a double-blind randomized multi-center trial." Journal of gastroenterology 29 (1994): 479-485.
- Gillen, Christine M., Rebecca J. Towers, David J. McMillan, Armando Delvecchio, Kadaba S. Sriprakash, Bart Currie, Berndt Kreikemeyer, Gurusharan S. Chhatwal, and Mark J. Walker. "Immunological response mounted by Aboriginal Australians living in the Northern Territory of Australia against Streptococcus pyogenes serum opacity factor." Microbiology 148, no. 1 (2002): 169-178.
- Courtney, Harry S., Yi Li, Waleed O. Twal, and W. Scott Argraves. "Serum opacity factor is a streptococcal receptor for the extracellular matrix protein fibulin-1." Journal of biological Chemistry 284, no. 19 (2009): 12966-12971.
- Low,D.,E., (2019) Steptococcus Pyogenes, Infectious Disease Advisor, January 19.
- Ramachandran (2019) Tropical Infections of The Heart- Special Focus On Rheumatic Fever And Endomyocardial Fibrosis With Clinical Perspectives, 2nd International Summit On Microbiology & Parasitology, Bangkok (Sukosal), Thailand, October, 24-25 (You Tube).


