
Research Article | DOI: https://doi.org/10.58489/2833-0951/006
Advisor doctor, Children Teaching Hospital of Baghdad Medical City and the National Training and Development Center.
*Corresponding Author: Aamir Jalal Al-Mosawi
Citation: Aamir Jalal Al-Mosawi (2022). Treatment of Williams syndrome: Evidence-based medicine and expert opinion. Biomedical and Biotechnological Sciences. 1(2). DOI: 10.58489/2833-0951/006
Copyright: © 2022 Aamir Jalal Al-Mosawi, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 July 2022 | Accepted: 25 July 2022 | Published: 08 August 2022
Keywords: Williams-Beuren syndrome, treatment, expert opinion.
Background: Williams syndrome which is also called "Williams-Beuren syndrome" is a mental retardation syndrome associated with aortic arch stenosis, and is generally results from deletion of chromosome 7q11.23. The syndrome has been recognized as early as 1961, but the associated neuropsychiatric abnormalities remained without specific treatment.
Williams syndrome which is also called "Williams-Beuren syndrome" is a mental retardation syndrome associated with aortic arch stenosis, and is generally results from deletion of chromosome 7q11.23. The syndrome has been recognized as early as 1961, but the associated neuropsychiatric abnormalities remained without specific treatment [1, 2].
The mother of an Indian boy with who received the diagnosis of Williams syndrome based on a genetic analysis consulted during June, 2022 us about the possible medical therapies. This paper reviews the relevant available evidence and synthesizes an expert opinion therapeutic protocol for the treatment of the boy [1, 2, 3, 4].
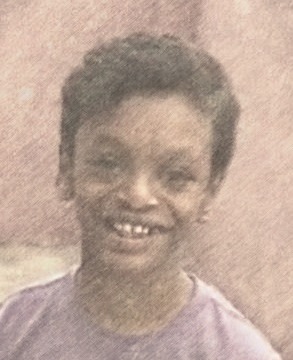
The boy was at about the age of eight years, and genetic analysis showed deletion of chromosome 7q11.23. The sketch in figure-1 shows the distinctive facial features which include wide mouth with prominent lower lip, puffiness around the eyes, and long upper lip length).
His condition was dominated by developmental delays, and cognitive impairment, but his speech was considered by the mother as good. His behavior was described as immature and impulse, and he was obsessed with the same topic discussions. Several videos of the child were studies and was found to have some autistic features as he was mostly not responding to name appropriately by turning to the sound and had poor eye contact. However, he was responding to questions and obeying simple instructions such as look at the camera. His walking was rather awkward with poor posture, and he could write up to 100 words, but poor writing and mathematics skills were poor. He was not described by the mother as a hyperactive boy. The boy also had mild drooling and was keeping his mouth open, but was closing it when asked to close it. His IQ was tested at 56.
Children with cognitive defect may also show occasionally poor response to name, but their good eye contact makes them different from autistic children. Therefore, this boy was considered to have mental retardation with some autistic features.
The mother was not aware of the development of hypercalcemia, but she reported that cardiac examinations showed mild aortic arch syndrome which didn’t interfere with his daily activities.
The mother emphasized the lack of benefit following a previous stem cell treatment.
Based on our extensive published experiences with treatment of mental retardation, autistic disorders, and other neurological, we recommended an initial therapeutic course which included:
1-Cerebrolysin 5ml ampoule (Stored and transported under 25 centigrade) given intramuscularly every third day during the morning hours (Not necessarily on the same time) [10 doses per month].
2-Piracetam (Nootropil) 5ml ampoule given intramuscularly every third day during the morning hours (Not necessarily on the same time, and not on the same day of cerebrolysin injection) [10 doses per month].
In 1961, John Cyprian Phipps Williams (Figure-2) and colleagues described four mentally retarded patients with supravalvular aortic stenosis (narrowing of the ascending aorta above the aortic valve) who had unusual facial features [1].

In 1962, Beuren and colleagues also described four mentally retarded patients with supravalvular aortic stenosis, and three of them had a striking facial resemblance. They emphasized the association of the aortic lesion with a systolic thrill and murmur mostly in the first right inter-costal space and beneath the clavicle [2]. In 1995, Nickerson et al reported that deletions of the elastin gene at 7q11.23 were observed in about 90% of Williams syndrome patients [3].
The occurrence of autistic features in patients with has been reported by Reiss et al as early as 1983 [4].
Cerebrolysin, a safe parenteral mixture of aminoacids which has been used with a benefit in a variety of childhood neuropsychiatric disorders, is the only medical therapy that is known to be associated with significant improvement and even cure of the major autistic features (Poor response to name and poor eye contact which indicate impaired communication) [5-11].
Parenteral piracetam has been used safely and with a benefit in a variety of childhood neuropsychiatric disorders, and it is one of the most important that have been used with benefit in mental and developmental retardation of various types and etiologies.
An expert therapeutic recommendation for the condition is described.
None.