
Research Article | DOI: https://doi.org/10.58489/2836-2292/008
1Dept of Respiratory Medicine, St Helier Hospital, Wrythe Lane, Carshalton, Surrey SM5 1AA
2Dept of Pharmacy, St Helier Hospital, Wrythe Lane, Carshalton, Surrey SM5 1AA
*Corresponding Author: Varney V.A
Citation: Ahmed S R B, Monir S, Sweeney S, Okin S, Lawrence R & Varney V.A, (2023). Salmon Calcitonin: A forgotten treatment for spine and pelvic fragility fractures; an audit of standard treatment versus Salmon Calcitonin. 2(1). DOI: 10.58489/2836-2292/008
Copyright: © 2023 Varney V.A; this is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 April 2023 | Accepted: 10 July 2023 | Published: 10 August 2023
Keywords: Fragility fractures, Salmon calcitonin, Pain control, Length of stay, Cost, Independence on discharge
Fragility fractures of the pelvis and spine cause significant pain and disability requiring a hospital length of stay of 15-45 days following which independence is often adversely affected. In 2018, the estimated cost to the NHS of such admissions was £4.4 billion per year. Fragility fractures are predicted to rise from the current 23% of the retired population to above 50% by 2030. This will place an enormous stress on NHS bed occupancy and subsequent home support if independence is affected. In 1961 the beneficial effects of salmon calcitonin (SCT) in treating fractures were first described and clinical trials confirmed its efficacy in reducing pain and accelerating fracture healing. This treatment option has now been largely forgotten as the focus has shifted to prevention by diagnosing and treating osteoporosis as per the National guidelines. In this quality audit we examined cases admitted with fragility fractures of the spine and pelvis from 1st Jan 2021-1st Jan 2022 and examined the recorded hospital admission and length of stay, treatments given and independence at discharge. When standard treatment (n=97) was compared with the patients also prescribed subcutaneous SCT (n=18) differences in outcome were seen. SCT treatment showed a 50% reduction in length of stay along with reduced requirement for powerful painkillers and 78% of these patients were discharged home without care requirements in comparison to only 18% on standard treatment alone. We discuss the audit findings and review the known data on SCT’s action and benefit in fragility fractures.
Osteoporosis is a disorder of reduced bone mass leading to bone fragility and fracture risk. The burden of this condition increases with advancing age and currently 1 in 3 women and 1 in 5 men over the age of 60years will suffer an osteoporotic fracture.
In the UK, the financial cost of these fractures is close to £4.4 billion per year and set to rise as the population ages along with costly hospital bed occupancy, radiographic imaging, pain relieving drugs, disability and home care upon discharge [1,2].
The mainstay of acute management is conservative with analgesia and physiotherapy despite its poor efficacy with lengthy hospital stay. This management contrasts with study data from salmon calcitonin use (SCT) in fragility fractures where pain control and fracture healing is accelerated and will be discussed from the results of this audit.
Vertebral compression fractures (VCF) predominately affect the T8-L4 region and frequently result in chronic back pain with loss of independence and height by 4mm for every affected vertebra [1].
Pelvic insufficiency fractures were 1st reported in 1982 where 3 cases of spontaneous pelvic fracture in severe osteoporosis resulted in incapacitating pain and disability despite minimal radiographic changes. Pelvic fractures currently affect 23% of the retired population but are predicted to increase to 60% by 2030 [2,3,4].
Triggers for fragility fractures
Include lifting, coughing, sneezing or low impact ground level falls with a hospital length of stay of 15-45 days. Box 1 shows risk factors [1].
Box 1: Causes of Fragility Fractures Advanced age Inactivity Steroid use Smoking Alcohol Intake Low Body Mass Index Female Sex Vitamin D deficiency Pelvic insufficiency post hip replacement |
Complications of Hospital admissions following fragility fractures
These include a myriad of complications such as pressure sores, chest or urine infections, venous thrombosis with embolic disease, muscle wasting, acute depression from pain and loss of independence. Traumatic pelvic fractures may cause pelvic haemorrhage with anaemia. Painkillers especially opiates, can give confusion, further falls, vomiting, constipation or even ileus. Patient mortality following a pelvic or VCF is increased by 14-27 % within 12 months with further increases with any additional fractures [2].
Diagnosis of vertebral and pelvic fractures
These are usually diagnosed from plain x rays although CT scans may be required if clinically suspected fractures are not visible on plain x rays (Figure 1).

Fig 1: Plain X-Rays showing: Arrows point to site of facture. (A) Pelvic Fracture, (B) Vertebral Compression Fracture
Differential diagnosis of fragility fractures
Awareness of the differential diagnosis is important as haematological disease such as myeloma, bony tumours, prostate cancer and osteomyelitis can produce fractures.
In younger people where osteoporosis is unexpected, detailed investigations are indicated including MRI scans, liver function tests, ESR, CRP, protein electrophoresis, Calcium, testosterone, oestrogen, parathyroid /thyroid hormones, renal function, Vitamin D levels and PSA [2].
Pain control in fragility fractures
The poor efficacy of standard pain killers (opiates and nonsteroidal anti-inflammatory drugs) in fragility fractures is well recognised and additional treatments such as a spinal brace or epidurals may be required along with lengthy physiotherapy and rehabilitation to recover some independence [5,6].
The Discovery of Salmon Calcitonin
Salmon calcitonin (SCT) is a polypeptide hormone consisting of 32 amino acids and was first discovered in 1961 and used for acute severe pain associated with fractures. It was noted to give particular benefit in VCF and pelvic fragility fractures. SCT is 40-50 times more potent than human calcitonin and has duration of action following its subcutaneous injection of several days which is far longer than its 24hr half-life [7,8].
Pain relieving effects of Salmon Calcitonin
SCT offers rapid and long-lasting analgesia that is superior to both opiates and non-steroidal anti-inflammatory drugs as shown in many clinical trials. Pain relief is generally achieved at 48hrs and treatment advised for 7-10days. SCT is associated with restored mobility by day 7 improving independence and quality of life. Studies of VCF + pelvic fracture show reduced pain on sitting standing and walking following SCT with earlier mobilization from its analgesic effects [9,10].
Mechanism of pain relief by Salmon Calcitonin
SCT has effects on the central nervous system which induces analgesia via multiple mechanisms. Animal studies demonstrate effects on the dorsal root ganglion and nerve sodium channels along with serotonin transmission. An intact serotonin system is needed to provide analgesia and to boost endorphins levels. All these mechanisms contribute to the pain relief by reducing transmission through central and peripheral nerves pathways. Avoiding specific serotonin antagonist drugs as shown in Box 2 is important as these can block the pain-relieving effect of SCT [11,12,13].
Box 2: Dosage schedule for salmon calcitonin (keep at 4°Cand use within 1 hr at room temperature) | |
Day 1 Day 2-10 | 50 units test dose subcutaneously 100 units subcutaneously daily Can reduce dose to 75 unit/day if excessive flushing or nausea following injection and give metoclopramide to treat nausea |
Check blood calcium is normal | Avoid starting Biphosphonates Add calcium and Vitamin D prescription for duration of treatment to avoid low calcium levels and ileus. SCT can be dosed alternate day if calcium levels are difficult to maintain |
Drugs that may reduce pain relieving effects of SCT | Ondansetron Tropisetron Naloxone Tramadol Tricyclics SSRI antidepressants MAOI antidepressants |
A meta-analysis of SCT’s analgesic effects in fractures confirms significant reductions in acute fracture pain at 7 days supporting its use on a short time basis [14,15]. There are many published studies with noteworthy benefit including one by Blau in 2003. This was a 14-day double-blind placebo-controlled study of 100 patients with acute VCF treated with subcutaneous SCT (100IU/day) or placebo. It showed reduced pain with restored mobility at day 4 in 47 of the 50 patients on receiving SCT. In the SCT-placebo group, 50 out of 50 patients were still bedbound despite standard pain relief at day 14 [13]. Similar data in pelvic fractures exists, demonstrating SCT’s efficacy in reducing severe pelvic pain that allows patients to rise from a chair, stand, walk and sit comfortably for long periods. This has major benefit to independence and SCT was associated with full radiological healing by week 7- 8 weeks compared with the control groups of >12.-13 weeks [16].
The administration of Salmon Calcitonin
In the UK, SCT is used subcutaneously, with intramuscular and intranasal treatments used in other countries. SCT has no known drug interactions itself although it may reduce blood lithium levels. It is well tolerated and deemed safe in older adults. Its main side effects following subcutaneous injection includes transient stinging at the injection site with possible flushing 20-30 minutes post injection that maybe associated with nausea and headache along with a temporary change in taste sensation. The dose can be reduced to 75 IU if nausea and headache persist. Since SCT is a polypeptide, allergic reactions are possible but rashes and hypersensitivity are extremely rare. Enquiry with regard to salmon fish allergy may be useful [8,13].
Indications and dosage of Salmon Calcitonin
SCT is licensed in the UK for acute fracture, bone loss from immobility, malignancy associated hypercalcaemia, Paget’s disease and osteoporotic fractures [14]. SCT must be kept in the fridge at 4oc and used within 1 hr at room temperature otherwise its activity is lost. See Box 2 for dosage schedule.
Uncorrected hypocalcaemia is a contraindication to SCT use. SCT will reduce blood calcium levels through its inhibitory effects on osteoclast activity along with increased stimulation of osteoblasts to repair bone requiring a significant calcium influx into the bone during repair. SCT also acts on the kidneys to reduce calcium reabsorption that lowers blood calcium levels further [8,14].
Patients with renal failure or other causes for hypocalcaemia should have blood levels corrected before SCT is commenced. Biphosphonates should be avoided at the time of SCT treatment as it may increase hypocalcaemia. A prescription for calcium with vitamin D3 2 tablets twice a day for the 7–10-day treatment period with SCT will usually be sufficient to maintain blood calcium levels in patients without renal failure.
This audit examined all patients admitted to the hospital Trust with a pelvic or spinal fragility fracture between Jan 2021-Jan 2022 under the ICD-10 codes of ICD-10-M80; ICD-10-S32.80; ICD-10-S32.00.
Data Collection
For each patient, a data sheet was completed recording admission and discharge dates, details of fracture site, risk factors and life style. Drug treatments used during the admission to control pain were recorded along with any additional treatments such as a spinal brace or epidural injection.
The hospital length of stay and independence at discharge including any requirement for a new package of care, residual /nursing home care or transfer for bed-based rehabilitation was noted as well as death during the hospital admission. The collected data was assessed and the outcome from standard pain control treatment and those who received the addition of SCT was compared.
Salmon Calcitonin treated patients
Patients treated with SCT were listed on the Pharmacy electronic prescription records as receiving SCT which acted as a cross-check of such cases and confirmed the number of doses received. SCT was dosed as shown in Box 2. Drugs that could reduce the benefit of SCT (Box 2) were avoided. The patients offered SCT were all admitted to wards under supervision of the doctors involved in this report. Since these doctors had past knowledge and experience of SCT treatment it was discussed with the patients and commenced to control pain and increase their mobility and independence.
Number of patients in the Audit
The ICD searches identified 235 admissions using the 3 search codes between Jan 2021-Jan 2022.
Data showed a total of 115 confirmed cases admitted with an acute pelvic or vertebral compression fracture requiring pain management; with the remainder representing old fragility fractures completely unrelated to the acute admission.
97 cases across the trust received standard care that was predominately pain relief and 18 cases received standard care with the addition of subcutaneous salmon calcitonin.
Group data Table 1: The results are summarised in table1.
Table 1: Data Cost of Inpatient care and discharge
| Salmon Calcitonin treatment (*SCT) | Standard pain relief treatment |
No. of cases | 18 | 97 |
Mean age (range) | 83 (58-94) | 83 (48-97) |
Percent female | 66% | 67% |
% Vertebral compression fracture | 45% | 81% |
% Pelvic fracture | 55% | 19% |
No. of *SCT injection (range) | 9 (4-16) | none |
Days to discharge (range) | 9 (4-16) | 16 (1-97) |
Died during admission | 0% | 7 (7%) |
Total No. of bed days used | 165 | 1548 |
Total cost of beds at £267 per day | £44,055:00p | £413,316:00p |
Total cost of bed per patient | £2,447:50p | £4,260:98p |
Discharge home without care | 14 (78%) | 17(18%) |
No. discharged with a new package of care at £700 per week | 2 (11%) | 54 (56%) |
Total cost of new package of care | £1400:00p | £37,800:00p |
No. discharged to residential/nursing home placement at £1000 per week | 0% | 16 (16%) |
Total cost of placement per patient per week | £0 | £16,000:00p |
No. discharged to bed-based rehabilitation at £900 per week | 2 (11%) | 3 (3%) |
Total cost of bed base rehab | £1800:00p | £2,700:00p |
Total of in-patient and discharge costs for group | £49,702:50p | £474,076:98p |
Total in-patient + discharge per patient | £2,761:25p | £4887:39p |
Both groups had a mean age of 83yrs with 33% male patients. Vertebral fractures were commoner (81%) in the standard care group compared with SCT group (45%).
SCT patients had a mean length of stay (LOS) of 9 days with a mean of 9 injections of SCT per patient. 14 patients (78%) were discharged home without a package of care (POC), while 11% required either a POC (n=2) or bed-based rehabilitation upon discharge (n=2).
For the standard pain relief only patients
the mean LOS was 16 days with 7% of patients dying during their admission. A new POC was required by 56% of discharged patients with 16% requiring a new residential or nursing home placement. Bed based rehabilitation was required by 3%. Only 18% were discharged home independent. Table1.
Drug treatments Table 2
The requirement for painkillers showed differences between the 2 groups. There was no requirement for morphine or oxycodone in the SCT group. Buprenorphine patches (10mcg) for slow background pain relief were used in 26% of all patients. The average drug cost per week for the standard pain relief patients was less than £10. Much greater drug costs were incurred for the SCT group at £373:16p per patient due to higher cost of SCT (100 units/day costing £368:00p for a 1-week course).
Table 2: Drug + treatments Prescribed
Weekly Cost of treatment | SCT patients % Requiring each drug | SCT cost for n=18 | Standard treatment % patients requiring each drug | Standard Treatment group cost for n=97 | |
| Paracetamol/cocodymal | £1.73 | 61% | £19-00p | 100% | £167-81p |
| Non steroidal anti-inflammatory drugs | £1.35 | 11% | £2-70p | 16% | £13-50p |
| Codeine Phosphate | £0.40 | 23% | £1-60p | 29% | £11-20p |
| Oramorph /Morphine Sulphate | £2.19 | 0% | - | 51% | £107-31p |
| Oxycodone | £6.00 | 0% | - | 14% | £78-50p |
| Tramadol | £0.50 | 5% | £0.50p | 8% | £4-00p |
| Buprenorphine patch | £3.14 | 27% | £15-70p | 26% | £78-50p |
| Lidocaine 5% topical patch | £17.50 | 17% | £52-50p | 12% | £192-50p |
| Gabapentin | £2.16 | 0% | - | 17% | £34-56p |
| Diazepam/lorazepam | £0.48 | 0% | - | 9% | £3-84p |
| Amitriptyline | £0.29 | 5% |
| 5% | £1.45p |
| Baclofen | £0.95 | 0% | - | 1% | £0.95p |
| Epidural | £16 | 0% | - | 2% | £32-00p |
| Spinal support brace | £50 | 0% | - | 2% | £100-00p |
| Salmon calcitonin | £368.00 | 100% | £6624-00p | 0% | - |
| Total cost | - | - | £6716-00p | - | £826-12p |
| Cost per patient | - | - | £373-11p | - | £8-51p |
Analysis of Cost for drugs, hospital stay and social care
Figure 2 shows the total cost per patient per week including the breakdown into inpatient bed occupancy costs, drugs costs and social care upon discharge.
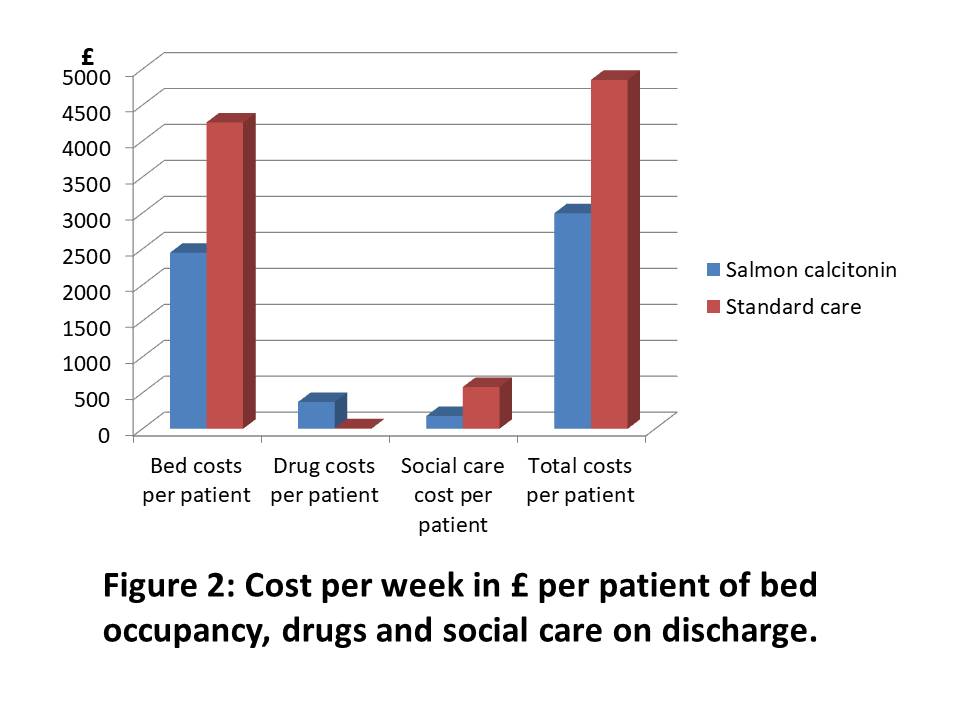
Fig 2: Cost per week in £ per patient of bed occupancy, drug and social care on discharge
The findings show a cost saving to the NHS for each of the 18 patients treated with SCT due to the reduced LOS and independence upon discharge that avoided costly home support or residential/nursing home placements. This saving amounted to £2,126.14p per patient per week with increased SCT drug costs clearly offset by the savings from reduced LOS and independence upon discharge. Although the SCT group represented only 19% of the total audit group data, the findings are similar to that reported in clinical trials.
The data shows earlier discharge for SCT-treated cases, with 78% independent at discharge contrasting with only 18% independent following standard pain control treatments. This offers significant potential cost saving for the NHS for just one condition that is set to rise with increasing pressures on the NHS and social care.
The authors found the total inpatient bed costs for just 97 patients in 1 hospital trust noteworthy at £413,316:00p with total social care for 1 week of £56,500:00p, clearly explaining the high annual NHS costs of £4.4 billion. Clearly hospital LOS for the standard care patients ranged between 1-97 days, while the SCT group range was 4-16 days despite the same mean age of the patients of 83yrs.
When these costs were divided by the number of patients, hospital costs with SCT were reduced by 57% and discharge costs by 56% per patient per week. This however does not take account of lengthy social care support after discharge that may be required long-term or even permanently within a residual or nursing home generating and much higher than home care as shown in table 1. This data does not address follow up by doctors, physical therapists or the ongoing requirement for pain-killers, nerve blocks, epidurals or even vertebroplasty in some cases.
Certainly, the powerful analgesic effects of SCT should not be overlooked in all fractures due to its superior efficacy for pain and fracture healing [7,15]. Fracture healing has great importance for survival in the animal kingdom, with rapid endochondral ossification required to produce a callus and woven bone to restore mobility and survival. There is good evidence for direct effects of calcitonin upon cartilage proliferation, callus formation and vascularisation in animal models. This is supported by biochemical, immuno-histochemical and radiological evidence with good quality bone that facilitates mobilization [16,17].
There are other analgesic properties of SCT that extend to neuropathic pain, phantom limb pain, migraines, post herpetic pain, osteoporosis, malignant bone deposits and Paget’s disease. Multiple rib fractures in patients with significant respiratory disease can be difficult to treat as opiates may produce significant respiratory depression in such patients. Here SCT can be lifesaving, as pain and healing is accelerated without evidence of symptom relapse upon cessation in published data [9,15,18,19].
The prevention of future fragility fractures needs urgent attention in view of the predicted increases over the next 10yrs. This first requires attention to risk factors, activity levels and vitamin D supplements, as levels that are known to be low in indoor workers [1]. Osteoporosis treatment needs to be optimised in those at risk. The discovery of the bisphosphonates had great advantages in osteoporosis, due to their long half-life and weekly oral dosage with proven osteoclast inhibition and anti-fracture efficacy over 3 years of approximately 30-50%. This led to a sharp decline in the prior use of SCT for osteoporosis leading it becoming largely forgotten. Many treatments are now available for this condition including various bisphosphonates, oestrogens and oestrogen receptor agonists, parathyroid hormone analogues and humanised monoclonal that reduces bone reabsorption via stimulation of Receptor Activator of Nuclear Factor Kappa-b ligand (RANKL-denosumab). Many of the newer treatment are limited to secondary care for patients whose bone mineral density remains low with use according to guidelines [20,21,22].
SCT use in acute fracture has been largely forgotten by most doctors. This data offers a reminder of the benefits of its pain relief and fracture healing properties with independence upon discharge offering a cost saving to the NHS. The predicted increase in fragility fractures within a decade may need a revival of this treatment to reduce overall costs for a common condition with great benefit for the treated patients.
We wish to thank the coding dept. for supplying the accurate search codes required and to the R&D dept. for searches on all admissions under those codes.