
Research Article | DOI: https://doi.org/10.58489/2833-0951/005
Advisor in Pediatric and pediatric psychiatry, The National Training and Development Center and Baghdad Medical City, Iraqi Ministry of Health, Baghdad, Iraq.
*Corresponding Author: Aamir Jalal Al-Mosawi
Citation: Aamir Jalal Al-Mosawi (2022). Prevalence of cryptorchidism in Iraqi school children and an educational review. Biomedical and Biotechnological Sciences. 1(1). DOI: 10.58489/2833-0951/005
Copyright: © 2022 Aamir Jalal Al-Mosawi, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 July 2022 | Accepted: 25 July 2022 | Published: 05 August 2022
Keywords: Prevalence, cryptorchidism, school children, Iraq.
Background: Isolated cryptorchidism without other abnormalities is the commonest congenital abnormality of the male genitalia. It is observed in about 1% of full-term infants at the age of one year. Little is known about the prevalence of the condition in Iraqi school children.
The term Cryptorchidism were derived from the Greek word “kryptos” which means “hidden” , and the Greek word orchis which means “testis”. The term Cryptorchidism used to describe the condition of the absence of a testis from the scrotum. Isolated cryptorchidism without other abnormalities is the commonest congenital abnormality of the male genitalia. It is observed in about 1% of full-term infants at the age of one year [1-10].
Screening of Iraqi school children for the presence of undescended testis (testes) during the year 2015 is described, and an educational review is presented in the discussion. The total male population in Baghdad during the year 2015 was 3997281 while the number of males under 15-year was 1510053.
Screening of Iraqi school children aged 6-14 year for the presence of undescended testis (testes) were performed during the year 2015 by the Iraqi Ministry of Health. 184852 school children were examined from 319 schools in Baghdad .3910 children (2.11%) had undescended testis (testes) including 30% with bilateral undescended testes, 33% with left undescended testis, and 37% with right undescended testis.
During embryonic life, the testes form near the mesonephric kidneys and move down the inguinal canal to the scrotum. Early during the seventh week of gestation, the testis-determining SRY gene on chromosome Y initiates the differentiation of the indifferent gonad into a testis.
At about the ninth weeks of gestation, Leydig cells produce testosterone to promote the development of the Wolffian duct into portions of the male genital tract. At the same time, the testis becomes a distinct organ with its distinct seminiferous tubules surrounded by vessels and encapsulated by the tunica albuginea. With the differential growth of the fetus, the testes move into the pelvis near the internal ring.
The testis remains in a retroperitoneal position until 28 weeks gestation when inguinal descent of the testes begins. Most testes descend into the scrotum by 40 weeks gestation.
Cryptorchidism which is the absence of a testis from the scrotum may result from: Stoppage of the descent of the testis along the normal path of descent (undescended or retractile testis). A testis moves off the normal path of decent (ectopic testis).
Death of a testis (absent testis) or non-development of a testis (atrophic testis).
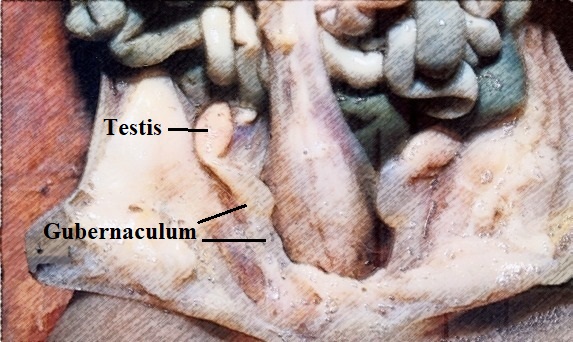
1-Gubernacular abnormalities: The gubernaculum testis is a structure connecting the lower part of the tunica vaginalis to base of the scrotum. The gubernaculum is involved in testicular descent through widening of the inguinal canal and guiding the testis down to the scrotum. 2-Reduced intra-abdominal pressures.
3-Intrinsic testicular or epididymal abnormalities.
4-Endocrine abnormalities including abnormalities in the hypothalamic-pituitary-gonadal axis. However, as cryptorchidism is commonly unilateral, endocrine anomalies are expected to be only partially responsible for the condition.
5-Anatomic abnormalities such as fibrous bands within the inguinal canal or abnormal arrangement of the cremasteric muscle fibers [1-10].
Baron Albrecht von Haller (Figure-1) and John Hunter (Figure-2) were probably the first to provide anatomical descriptions of cryptorchidism [5, 6].
Baron Albrecht von Haller described the abdominal position of the fetal testis in his well-known publication “Opuscula Pathologica” published in 1755. Baron Albrecht von Haller reported the presence of abdominal testis, but he couldn’t not know the accurate timing of testicular descent. However, his explanation of the process of testicular descent was not correct [5].
The work of Baron Albrecht von Haller attracted the interest of John Hunter, who made important observations. John Hunter was regarded as one of the fathers of modern surgery and also of anatomy [6].
John Hunter studied the descent of fetal testis as he became interested in Baron von Haller's observations. In 1762, Hunter verified the abdominal position of the fetal testes. Postmortem dissection helped John Hunter to determine the timing of testicular descent at around the eighth month.
John Hunter also described the retractile testes, undescended testes, and testicular ectopia. He disagreed with the ideas that the testis is forced into the scrotum by the compressive force of respiration, or pulled by the cremaster muscle. The structure of the gubernaculum, or genito-inguinal ligament, was first described and named by Hunter in 1762.
He emphasized the significance of gubernaculum as a helm or rudder for testicular descent. Hunter's precise description of fetal testicular descent contributed significantly to the understanding of cryptorchidism. John Hunter emphasized the need for treatment of undescended testis after a period of observation [6].
The gubernaculum (Figure-3) is an embryonic structure arises in the upper abdomen from the lower end of the gonadal to guide the testis in it's descent to the inguinal region [6, 7, 8].
The ideas of surgical correction of the undescended testis appeared early in the 1800s, and the theoretical bases for the need of orchiopexy in patients with cryptorchidism originated from the work of the two pioneers in the 18th century, Baron Albrecht von Haller and John Hunter [5,6].
In 1871, James Adams from London Hospital in 1871 suggested the need for surgery for undescended testis, but he couldn’t perform successful surgery. He thought that undescended testis is associated with poor scrotal development, increased risk of atrophy, and susceptibility to injury [7].
In 1840, Thomas Blizard Curling (Figure-4) described the gubernaculum as a soft, solid protruding body with variable shape and size at different stages of testicular descent. He thought that the gubernaculum terminates in three muscular processes, before, during and after testicular descent including:
A-External connected to Poupart's ligament.
B-Middle through the external ring to the bottom of the scrotum.
C-Internal to the os pubis and the rectus muscle sheath.
Thomas Curling published a review in 1866 on undescended testicles in his book entitled “A Practical Treatise on the Diseases of the Testis”. He also reviewed the possible causes of the retained testicle including the defective development of the cremasteric muscle, adhesions secondary to peritonitis, and a contracted external ring. The work of Curling included some misconceptions. However his observations provided a theoretical background for orchiopexy [8, 9]

As the gubernaculum contains muscle that contract, Lockwood Charles Barrett (Figure-5) suggested the traction theory of testicular descent. After examining eight fetuses from seven weeks gestation to full term, he reported the change of distal gubernaculum from a soft, jelly-like mass into a leash of fibers that spread out to several areas and pulling the testis into the scrotum [10].
The first successful orchiopexy was performed by Thomas Annandale (Figure-6) in 1877. Orchiopexy (orchidopexy) is surgically moving and fix a testis into the scrotal sac [11].

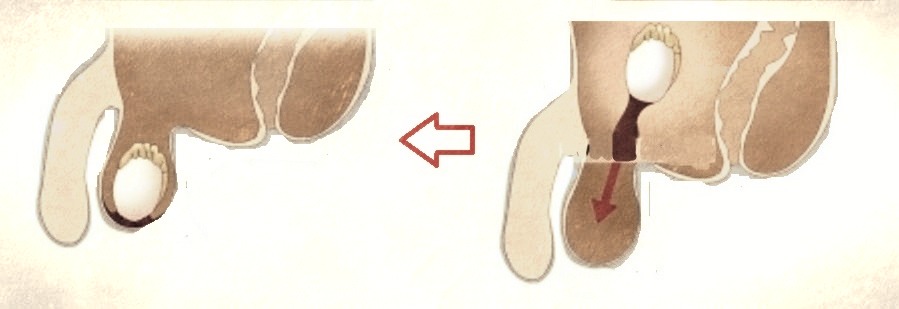
Annandale was who was born on February, 2, 1838 .He treated successfully a three-year-old boy who an ectopic testicle surgically. Annandale reported the first successful orchiopexy in a boy who had a right ectopic testis palpated on ipsilateral perineum. He performed the operation on the fifth of July; 1877.He freed the testis and gubernaculum from its attachment, and brought the testis to the scrotal sac (Figure-7) [11].
The work of Max Schüller, Arthur Dean Bevan (Figure-8) and their descriptions of the principles of testicular mobilization, separation of the processus vaginalis, and re-locating the testis into the scrotal sac in 1881, and 1899 respectively contributed significantly to establishing the current techniques for standard orchiopexy[12,13,14].
Simşek et al (1995) from Istanbul examined 6381 male primary school children in Turkey during the years 1990 and 1991. Undescended testes were found in 91 boys (1.43%) suggesting a prevalence of 14.3/1000 primary school children [15]. Inan et al (2008) from Edirne in Turkey examined 1500 children and reported a prevalence of undescended testes of 7.3/1000 children [16].
Okeke and Osegbe (2001) from Lagos in Nigeria examined 1096 boys (aged 5-13 years) from five primary schools for undescended testes. They found unilateral cryptorchidism in nine children (4 left sided and 5 right sided) suggesting a prevalence of 0.82% (8.2/ 1000[17].
Little is known about the prevalence of cryptorchidism in school children in many geographic regions in the world. However, the prevalence of cryptorchidism in Iraqi school children was estimated during the hear 2015 at 21/1000, which is much higher than the previously reported in Turkey and Nigeria.
None.