
Research Article | DOI: https://doi.org/10.58489/2837-3332/004
1 Academic scholarship of the Department of Obstetrics, University of Western Macedonia
2 PhD candidate, Department of Obstetrics, University of Western Macedonia
3 Cognitive psychologists
4 PhD Cognitive Psychology, Neuropsychologist of C’ Department Psychiatric Clinic of HEPA Hospital Thessaloniki
5 Professor, of C’ Department Psychiatric Clinic of AHEPA Hospital Thessaloniki
6 Professor, Director of C’ Department Psychiatric Clinic of AHEPA Hospital Thessaloniki
7 Professor, Directeur du laboratoire CAPS (Cognition, Action, et Plasticité Sensorimotrice), Université de Bourgogne, Dijon France.
8 Psychiatrist Consultant, 3rd Psychiatry Department of the Aristotle University of Thessaloniki, University General Hospital of Thessaloniki, AHEPA.
*Corresponding Author: Theofilidis Antonis
Citation: Theofilidis Antonis, Savvidis George, Sofologi Maria, Hanopoulou Margarita, Tsagaridis Konstantinos, et.al., (2023). Assessment of Mental Imagery of Movement in Schizophrenia. Journal of Clinical Surgery and Reports. 1(1). DOI: 10.58489/2837-3332/004
Copyright: © 2023 Theofilidis Antonis, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 March 2023 | Accepted: 23 March 2023 | Published: 31 March 2023
Keywords: schizophrenia; mental imagery of movement
Schizophrenia patients often present with neurological signs such as left/right confusion, impaired coordination of movements, and motor abnormalities may occur secondary to antipsychotic medications. Neuropsychological tests identify various dysfunctions, such as difficulty in focusing attention, difficulty in abstract thinking or difficulty in changing the response frame, while Neurophysiological tests show slowing down of reaction time, problems with eye tracking, etc. There are no studies in the international literature dealing with the investigation of mental imagery of movement in Greek patients with schizophrenia. Also, the position that patients with schizophrenia – regardless of their symptom profile, age, sex, and chronicity of the disease – have a permanent difficulty in creating and manipulating an internal model of their movement prediction, has not been substantiated enough to date.
Aim: In the present study we examine the function of visual-motor coordination and the time to achieve the goal-directed movement of the dominant hand of patients with schizophrenia
Method: The sample we used in our research consisted of patients with diagnosed schizophrenia and healthy individuals. Schizophrenia patients belonged to the experimental group and healthy subjects to the control group. The number of examined patients was 39 and the healthy 51. the assessment of the movement and its mental representation was carried out with the real and mental movement of the dominant hand between two square targets located at a distance of 20 cm, on white paper of A4 size.
Conclusions: Visuomotor coordination of a specific hand movement differs between patients with schizophrenia and the normal population. In particular, the means of the goal-directed hand movement achievement time in the actual execution condition and in the mental execution condition of the patients were significantly higher than the corresponding times of the standard population.
Neuropsychological deficits are recognized as primary symptoms of psychotic disorders, since they are detected even in the early stages, with some of them showing a more significant decline (e.g., executive functions, memory, attention) and others a smaller but significant one (e.g., language, movement perception, psychomotor). A wealth of neuropsychological research over the past decade has contributed to elucidating the nature and significance of cognitive dysfunction in schizophrenia. Today we know that patients with schizophrenia show lower performance in all known neuropsychological tests compared to healthy controls.
We know that schizophrenia is governed by deficits in psychomotor speed (Ekerholm et al., 2012; Schretlen et al., 2007). Psychomotor speed refers to the time to process a stimulus, prepare the response to that stimulus, and execute the response (Ekerholm et al., 2012). It has been shown that patients with schizophrenia are disadvantaged compared to healthy individuals in tests of psychomotor speed (Ekerholm et al., 2012. McIntosh et al., 2005. Schretlen et al., 2007). However, this difference does not always reach the significance level (Bozikas et al., 2006). Of interest is the result of the research by Riley and his colleagues (2000) that deficits in psychomotor speed in schizophrenia appear as early as the first episode, reinforcing the view that this area is greatly damaged by the presence of psychotic symptoms (Townsend & Norman, 2004). Sweeney et al.'s (1991) study found improvement in psychomotor speed in both first-episode schizophrenia patients and patients with a previous history of psychosis (Rund, 1998), which is consistent with the view that neurocognitive deficits in patients with schizophrenia remain relatively stable across the lifespan (Ekerholm et al., 2012; Townsend & Norman, 2004).
Movement imagery is a mental process in which a specific movement is internally simulated without actually performing the movement. According to simulation theory, mental movements are essentially movements that do not take place (Jeannerod and Decety, 1995; Jeanmann, 2001). Much research has highlighted the relationship between real movement and its corresponding mental representation as well as common brain areas that are activated during planning and execution in both cases, while both mental and real movement follow the same rules (e.g., speed-accuracy, speed-curvature relationship) and maintain the same temporal structure (Decety and Jeannerod, 1995; Maruff et al., 1999; Bakker et al., 2007; Gueugneau et al., 2008; Papaxanthis et al..,2012). In addition, mental training improves motor performance (Yaguez et al., 1998; Gentili et al., 2006, 2010; Avanzino et al., 2009) and enhances muscle strength (Yue and Cole, 1992; Zijdewind et al., 2003; Ranganathan et al., 2004).Neuroimaging studies have revealed a common activation of specific brain regions during both motor and mental execution of a movement (parietal and prefrontal cortex, primary cortex, basal ganglia and cerebellum) (Jeannerod, 2001; Guillot and Collet, 2005; Szameitat et al., 2007; Munzert et al., 2009; Hetu et al., 2013).
Research using movement imagery tests is a useful and sensitive method of investigating the unconscious process of representation (Jeannerod and Decety, 1995). Movement imagery has been widely used to investigate the movement system in both healthy and clinical populations. The advantage of investigating kinesthetic imaging is that the internal processes of real movement that involve planning and planning can be studied. This element is very important for the study of the production and execution of the movement and the related deficits shown by patients of various categories such as patients with psychiatric or neurological syndromes. In these patient cases the ability or inability to produce or perform a movement can indicate whether the relevant brain function has begun to be affected, to what extent it is deficient, and the degree of progressive impairment.
Deficits in mental imagery of movement have been assessed in Parkinson's disease (Dominey et al., 1995; Helmich et al., 2007; Heremans et al., 2011), prefrontal cortex syndrome (Kagerer et al., 1998), motor - sensory cortex (Sirigu et al., 1996; Danckert et al, Malouin et al., 2004), and in multiple sclerosis (Heremans et al., 2012; Tacchino et al., 2013). Investigating the mental imagery of movement also helps psychomotor retardation (Psychomotor retardation -PMR-) which is a central factor in the assessment of clinical and therapeutic effects and can seriously affect the psychosocial functioning of patients. Psychomotor rehabilitation modifies all of the person's actions, including mobility, mental activity, and speech (Widlocher, 1983).
Kinetic imagery is about being able to create internal/mental images before they are executed. Patients with schizophrenia have difficulty accurately tracking mental images of movement, and are unable to produce accurate mental images of their own movements. Research has shown that many of the first-order symptoms of schizophrenia, for example delusions of control in which the patient believes that external forces are controlling their thoughts or actions, can be characterized as deficits in reality monitoring or self-monitoring of internally generated thoughts. For the schizophrenic patient a self-control deficit, which manifests as an inability to recognize his thoughts or actions as his own, is also auditory hallucinations when these manifest as an inability to recognize inner speech as self-generated. However, patients with schizophrenia are a heterogeneous group of patients with deficits in attention, memory, and executive functions.
Thus, a difficulty to examine the hypothesis that they present difficulties and deficits in motor mental imagery, is the use of neuropsychological tests that usually concern cognitive abilities (such as attention and memory) that in one way or another are presented as deficits in this group of patients. From a neuropsychological point of view the parietal cerebral cortex is an interesting area for research in patients with schizophrenia, since it receives information from multiple sensory inputs, is crucial for the control of directed limb and eye movements, and plays an important role in proprioception (somatotopographic recognition). The two brain regions of the parietal cortex are involved in different cognitive functions with the left region involved in speech and movement processes, and the right region involved in processing spatial representations and focusing attention on specific environmental stimuli. Previous research has shown deficits in eye movement control and visual attention in patients with schizophrenia, suggesting deficits in parietal lobe function (Delerue et. al., 2013).
Frontal and parietal brain structures play an important role not only in the control and execution of goal-directed movements but also in the ability to recognize movements as individual. Neuroimaging studies investigating the recognition of self-generated movements versus other movements have shown increased activation in regions of the parietal and frontal cortex that are critical for the control of goal-directed movements. Interestingly, when hallucinating schizophrenics are asked to discriminate between self-made hand movements and movements of a "foreign" hand, they mistake the foreign movements as their own in 80% of trials (Delerue et. al., 2013). Also, the conscious control of certain movements for patients with schizophrenia presents particular difficulties(Delerue et. al., 2013). However, the question that has not been sufficiently answered to date is whether these difficulties are exclusively related to visual feedback of information or are related to a central deficiency in the ability to visually motor coordination for the execution of goal-directed movements of patients with schizophrenia. Motor mental imagery presupposes the creation of an internal mental image of a movement and its mental projection with successive individual images of the intended action (Delerue et. al., 2013). Tasks requiring motor imagery are a good means of studying goal-directed movement for patients with schizophrenia as well. Typically, when subjects are asked to imagine a movement at a mental level the time required to mentally perform that movement will be the same as the time to actually perform the movement (Delerue et. al., 2013).
Research case
Based on the preceding literature review, it became clear that patients with schizophrenia present many cognitive deficits, the most important of which are related to executive functions, memory, and attention. The aim of our own research was to investigate the target-directed movement ability of the dominant hand of schizophrenics and to compare this ability with healthy individuals in order to clarify the possible difference between the two groups. Our research question has not been answered in any research in the Greek area and we hope that it will be another important element in being able to clarify with the greatest possible precision the deficits in the cognitive functions of schizophrenic patients.
Sample
The sample we used in our research consisted of patients with diagnosed schizophrenia and healthy individuals. Schizophrenia patients belonged to the experimental group and healthy subjects to the control group. The number of patients examined was 39 and the healthy 51. The age range of the patients was from 28 to 64 years with a mean age of 45.3 years. Nine were men and six were women. Seven had completed secondary education, five tertiary and three primary. The group of healthy subjects was matched based on all the above elements with the group of schizophrenics. All participants had normal vision and were right-handed. The patients had previously been treated at the 3rd University Psychiatric Clinic of the ACHEPA Hospital in Thessaloniki and participated in the study during their scheduled visit to the clinic's outpatient clinics. Exclusion criteria from the study were: depression, neurological disease, severe organic disease, substance use. Also, those patients receiving medication (Haloperidol, Risperidone, Biperidone) which can affect movement were excluded. The patients in the sample were receiving second generation antipsychotics (Second Generation Antipsychotics SGAs – Clozapine up to 900mg/24h, Olanzapine up to 20mg/24h, Aripiprazole up to 30mg/24h, Cariprazine up to 6mg/24h, Amisoulpride, Lourasidone, Ziprasidone). Control group participants were free from any neurological, cognitive and organic impairment and were randomly selected from the community. All participants gave written consent to participate in the study. The research protocol was approved by the Ethics Committee of the Faculty of Medicine of the A.P.Th. and conducted in accordance with the principle set out in the Declaration of Helsinki.
Object of the study - research questions
In the present study, the function of visual-motor coordination and the time to achieve the goal-directed movement of the dominant hand of patients with schizophrenia was investigated. The questions to be answered were:
The hypotheses of the research
Data collection method - experimental protocol.
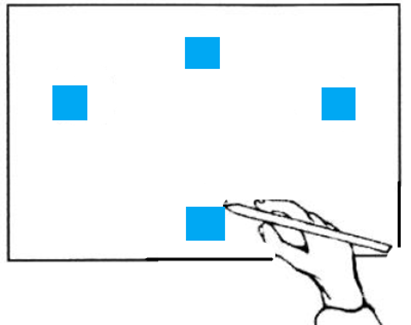
Data collection took place in a quiet office. In order to limit the influence of circadian rhythms on motor and mental performance (Gueugneau et al., 2009; Gueugneau and Papaxanthis, 2010), all experiments were performed in the morning (between 9 and 11 AM). Participants were seated comfortably in an adjustable chair in front of a table whose edge was aligned with their chest at the level of the diaphragm. In the middle of the table, the pieces of paper (A4 format) were placed at a distance of 20 cm from the chest of the participants. Three targets (black squares) and a starting point (abference) were printed on each sheet. We used four different target sizes (0.5 cm, 1 cm, 1.5 cm, 2 cm) and the distances between the targets were (15 cm) to model the test according to Fitts' law (Fitts, 1954).
Participants had to perform (actual movement) or imagine themselves performing the movement (mental movement) between the targets as accurately and as quickly as possible (i.e., we adapted Fitts' law motor paradigm, see also Maruff et al. (1999) and Gueugneau et al., while the presentation of the targets was randomized to exclude the learning process. After the instructions were briefed and explained, participants were free to initiate the real or mental movements when they felt ready. /s. Each real or mental movement was performed eight times between targets for each trial (0.5 cm, 1 cm, 1.5 cm, 2 cm). For mental movements, participants were asked to place their pencil over the original target (starting point), hold it still throughout the trial, and feel that they are performing the task (motor) as they would in reality. of a movement at the mental level is a necessary condition for the motor system to be involved (Stinear et al., 2006; Gueugneau et al., 2013). For each actual test, we measured the reaching time as well as the accuracy of the movements.
Participants were told that if they missed more than two targets during a trial, it would be canceled (invalid trial) and repeated at the end of the session. No tests had to be repeated. Each test was performed on separate sheets. The main experiment was preceded by a series of practice trials, which allowed participants to familiarize themselves with the task. The targets used in practice were of different sizes (3 cm and 2.5 cm) than those used in the experiment. After this practice phase, all participants verbally reported that they were able to generate motor imagery after having practiced 9–10 times. During the experiment, all participants performed eight real and eight mental trials for each different target dimension (64 trials per participant) in random order. When participants completed eight consecutive trials, they rested for ∼1 min to avoid physical and mental fatigue. After achieving the experimental protocol, none of the participants reported mental or physical fatigue and any difficulty in internally simulating the movements.
Regarding gender, the sample consists of 42 men (46.7%) and 48 women (53.3%). Regarding the disease, 51 normal (56.7%) and 39 patients with schizophrenia (43.3%) participated. Of all the participants in the research, 2 people had completed primary education (2.2%), 12 people (13.3%) high school, 23 people high school (25.6%) 37 people (41.1%) the university while 16 people had also completed postgraduate education (17.8%). 27 people (30%) were aged 19 to 29, 19 people (21%) were aged 30 to 39, 12 people (13%) were aged 40 to 49, 23 people (26%) were aged 50 to 59 and 9 people (10%) belonged to the age group of 60 to seventy years.
Control of performance averages
We calculated the averages of the time to achieve the specific goal-directed real and mental movement to targets of different dimensions (square targets with dimension: 0.5X0.5 cm, 1X1 cm, 1.5X1.5 cm, and 2X2 cm). Testing the means with the t-test for independent samples showed that reaching time was significantly associated with schizophrenia in all cases (real and mental movement and different goal dimensions). Patients with schizophrenia perform this movement in a longer period of time than the normal population.
| Patients | Normal |
|
Actual movement – target 0.5X0.5 cm | Μ=34,97, SD=9,797 | M=18,57, SD=6,152 | t=60,215 p=.000 |
Actual movement – target 1X1 cm | Μ=30,21,SD=8,408 | M=15,96, SD=4,927 | t=57,563 p=.000 |
Actual movement – target 1.5X1.5 cm | Μ=27,46, SD=6,95 | M=14,57, SD=4,041 | t=57,25 p=.000 |
Actual movement – target 2X2 cm | Μ=25,67,SD=7,432 | M=13,53, SD=3,733 | t=52,59 p=.000 |
|
|
|
|
Μental movement – target 0.5X0.5 cm | Μ=25,28, SD=7,96 | M=15,39, SD=4,133 | t=53,55 p=.000 |
Μental movement – target 1X1 cm | Μ=24,62, SD=7,738 | M=14,90, SD=4,016 | t=53,54 p=.000 |
Μental movement – target 1.5X1.5 cm | Μ=23,31, SD=6,795 | M=14,04, SD=3,873 | t=56,573 p=.000 |
Μental movement – target 2X2 cm | Μ=23,31, SD=7,179 | M=13,55, SD=3,786 | t=54,025 p=.000 |
Τhe execution time of both real and mental movement in all subtests (target size) is longer for patients with schizophrenia compared to the corresponding times of normal subjects.
As the dimension of the target increases, the time to achieve the movement decreases for both conditions (real and mental movement) and for both groups (normal population - patients with schizophrenia).
Schizophrenia patients show larger differences between the mean execution time between the actual and mental execution of the movement than the corresponding differences of the normal population.
Τhe difference in the averages of the time to achieve the movement is smaller between the two groups (normal - schizophrenic) for the condition of mental execution of the specific movement.