
Case Report | DOI: https://doi.org/10.58489/2836-8630/007
*Corresponding Author: Asmir Jonuzi
Citation: Asmir Jonuzi, Zlatan Zvizdić, Sadeta Begić Kapetanović, Emir Milišić, Ajla Buljubašić, (2024). An atypical presentation of a patient with a combination of omphalomesenteric duct related anomalies: A case report, Journal of Clinical Peadiatrics and Care. 2(1). DOI: 10.58489/2836-8630/007
Copyright: © 2024 Asmir Jonuzi, this is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 August 2023 | Accepted: 02 February 2024 | Published: 07 February 2024
Keywords: Vitelline duct, Meckel's diverticulum, Omphalomesenteric cyst.
The omphalomesenteric duct is an embryonic structure which connects the yolk sac to the midgut. The omphalomesenteric duct attenuates between the 5th and 9th week of gestation. Failure of the omphalomesenteric duct involution, either partial or complete, results in various omphalomesenteric duct remnants including Meckel's diverticulum, patent vitelline duct, fibrous band, sinus tract, umbilical polyp and cyst. Omphalomesenteric duct remnants are present in 2% of the population but related diseases have seldom been reported in children. We present a case of a 12 years old boy there was coexistence of the previously mentioned anomalies of the omphalomesenteric duct (Meckel's diverticulum, sinus and cyst). To our knowledge, our case is the first pediatric case with the coexistence of the previously mentioned anomalies of the omphalomesenteric duct.
The omphalomesenteric (vitelline) duct is an embryologic structure that acts as a communicating tract between the yolk sac and primitive midgut during early embryonic development [1]. Between the fifth and seventh week of gestation, the omphalomesenteric duct normally obliterates. If there is any disruption in this process, it will result in omphalomesenteric duct anomalies that include a wide variety of clinical entities such as Meckel’s diverticulum, fistulas, sinus tracts, cysts, umbilical polyps and fibrous bands. The most common of these anomalies is Meckel's diverticulum for which the popular „rule of 2s “most often applies: it is found in approximately 2% of the general population, it is usually located 2 feet proximal to the ileocecal valve and is approximately 2 inches in length, it can contain 2 types of ectopic tissue - pancreatic or gastric, it is generally present before the age of 2 years, and it is found twice as commonly in males [2,3]. The possible complications of Meckel's diverticulum include perforation, vesicodiverticular fistula, ulceration, hemorrhage, intussusception, intestinal obstruction from attached bands and tumors [4]. The simultaneous presence of the sinus tract, omphalomesenteric cyst, and Meckel's diverticulum has never been reported in children.
We present a case of a 12-year-old boy there was the coexistence of the previously mentioned anomalies of the omphalomesenteric duct.
A 12-year-old boy presented with abdominal pain, nausea and vomiting. On physical exam, the patient was alert, afebrile, eupneic, euhydric, with a pulse of 113 bpm, blood pressure 119/62 mmHg, and oxygen saturation of 100% on room air. Also, he had impaired mobility due to pain. The abdomen was soft, and painful to palpation in the lower quadrants, especially in ileocaecal region. Psoas and obturator signs were negative. Murphy's punch sign was also negative. An abdominal ultrasound was suggestive of acute appendicits. Baseline laboratory studies drawn were notable for a leukocytosis of 15,4 with a neutrophilic predominance (88,1%). Monocytes, lymphocytes and
eosinophils were low. C-reactive protein was 9,0 mg/mL. The blood tests, ectrolytes and other parameters were in a normal range. After evaluation by a pediatric surgeon, the patient was indicated for emergency surgery due to suspicion of acute appendicitis. The laparatomy, carried out through a McBurney's incision, evidenced a fixed cecum, and retrocaecal appendix with a normal diameter. In a distance of 30-40 cm from the ileocaecal valve, Meckel diverticulum was found that originated from the antimesenteric side of the ileum and connected by a sinus in cystic dilatation which was fixed for the inner side of the umbilicus (Figure 1).
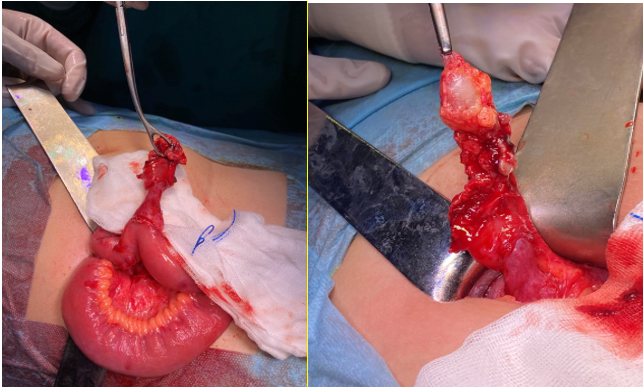
After the tumorous formation cyst was separated from the umbilicus, partial ileal resection was performed and intestinal continuity was restored via single layer ileoileal anastomosis (Figure 2).

An appendectomy was also performed. Post-operative course was uneventful, the patient did well and was discharged home on 7 th post-operative day.
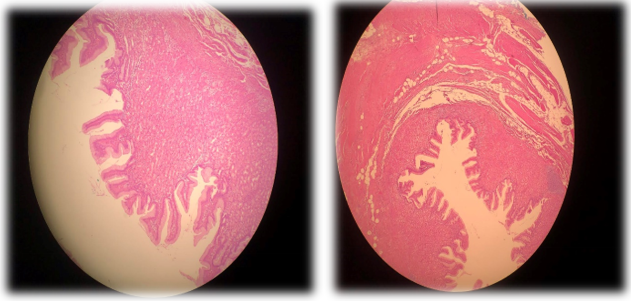
Pathohistological examination of the excised diverticulous formation with a cystic enlargement showed histological picture of true diverticulum that consists of all layers of intestinal wall with mixed inflammatory infiltrate in the lamina propria and ectopic gastric mucosa (Figure 3)
The omphalomesenteric duct, also called vitelline duct, is an embryonic structure which connects the primitive yolk sac to the primitive midgut, through the umbilical coelome, and contains the omphalomesenteric vessels which provide nutrition to the early developing embryo until the placenta is established [5]. The omphalomesenteric duct gradually attenuates as the placental circulation is increasing and atrophies, separates from the intestine and finally disappears between the 5th and 9th week of gestation [6]. Partial or complete failure of involution of the omphalomesenteric duct results in various residual anatomical entities (Figure 4) [7].

Although Meckel's diverticulum is the most common presentation of an omphalomesenteric duct remnant and is generated when the proximal duct persists [7,8]. However, it rarely gives rise to symptoms and its discovery is usually accidental [9].
The time required to reach a correct diagnosis of of Meckel’s diverticulum before surgery is often difficult because a complicated form of this condition may be clinically indistinguishable from a variety of other intraabdominal diseases such as acute appendicitis, inflammatory bowel disease, or other causes of small bowel obstruction [10].
In cases the entire duct remains patent, an omphalomesenteric fistula is formed between the umbilicus and the ileum, while a persistent lesion of the distal duct forms a sinus tract and the patency of the intermediate duct with closure at both ends leaves an omphalomesenteric cyst [11]. Ultimately, a fibrous ligament may be present with no open fistulas connecting the umbilicus to the intestine [11].
In the present case, the entire omphalomesenteric duct has remained, but forming a patent fistula, it presented with a sinus tract communicating with an omphalomesenteric cyst, which was connected by a sinus to a Meckel's diverticulum, a coexistence of multiple omphalomesenteric remnants that has, according to authors' knowledge, never been reported.
Clinical presentation of omphalomesenteric remnants includes abdominal pain, intestinal obstruction, rectal bleeding, umbilical hernia and umbilical discharge and the symptoms are age dependent and usually occur before the age of four, while adult patients are usually asymptomatic [6,7,12]. Ultrasound, CT scan, Meckel's scan and fistulograms help determine the cause of the symptoms, when the presence of omphalomesenteric duct remnants is suspected [13].
In conclusion, we presented a rare case of a boy with concurrent omphalomesenteric cyst, sinus and Meckel's diverticulum, who underwent surgery mimicking acute appendicitis. Preoperative diagnosis is often difficult. The presence of a periumbilical cyst in a young adult with previous episodes of cramping abdominal pain without obstruction should raise suspicion of remnant OMD as the underlying etiology.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest